*Marzena Kesler1, Aleksandra Koch1, Magdalena Rychlik1, Jacek Bierca2, Małgorzata Kołodziejczak2, 3
Assessment of the rationale for the use of preventive antibiotic (clindamycin) therapy in patients operated on for anal fistula based on authors’ own experience
Ocena zasadności stosowanej profilaktyki antybiotykowej (klindamycyny) u pacjentów operowanych z powodu przetoki odbytu w materiale własnym
1Laboratory of Diagnostic Microbiology, County Hospital in Ostrów Mazowiecka
2Department of General Surgery, County Hospital in Ostrów Mazowiecka
3Warsaw Proctology Center, St. Elisabeth Hospital, Mokotów Medical Center, Warsaw
Streszczenie
Wstęp. Od wielu lat za podstawową przyczynę powstania przetoki odbytu uważa się infekcję bakteryjną gruczołów odbytu. Inne przyczyny to przede wszystkim choroby zapalne jelit: choroba Leśniowskiego-Crohna, wrzodziejące zapalenie jelita grubego, wszelkie stany obniżenia odporności związane m.in. z infekcją wirusem HIV, przyjmowaniem leków immunosupresyjnych, ciała obce, urazy. Niewiele jest prac analizujących rodzaj patogenu bakteryjnego w powstaniu przetoki odbytu, co więcej, wydaje się, że pomimo iż podstawowym leczeniem choroby jest postępowanie chirurgiczne, pomija się znaczenie leczenia infekcji kryptowej oraz zgodnej z posiewem antybiotykoterapii.
Cel pracy. Celem badania była ocena zasadności stosowanej profilaktyki antybiotykowej (klindamycyny) u pacjentów po zabiegach proktologicznych.
Materiał i metody. W okresie od 1 stycznia do 31 grudnia 2019 roku na Oddziale Chirurgii Ogólnej Szpitala Powiatowego w Ostrowi Mazowieckiej zoperowano 46 pacjentów (40 mężczyzn, 6 kobiet) w wieku od 28 do 71 lat (śr. 49 lat) z powodu przetoki odbytu. Wszyscy pacjenci byli operowani przez tego samego operatora, doświadczonego w wykonywaniu operacji proktologicznych. U wszystkich pacjentów pobrano w trakcie operacji materiał na posiew bakteryjny oraz zastosowano profilaktykę antybiotykową w postaci klindamycyny 2 x 600 mg i.v.
Wyniki. Duża liczba wyhodowanych bakterii Bacteroides spp. wykazała wysoką oporność na klindamycynę (88% oporności). Grupa bakterii beztlenowych wykazała oporność na klindamycynę rzędu 60%.
Wnioski. 1. Klindamycyna nie powinna być stosowana w profilaktyce antybiotykowej u pacjentów operowanych z powodu przetoki odbytu na Oddziale Chirurgii Ogólnej Szpitala Powiatowego w Ostrowi Mazowieckiej. 2. Należy brać pod uwagę zmienną wrażliwość bakterii na antybiotyki i zmieniać profilaktykę antybiotykową w zależności od wytworzonej oporności na kolejne stosowane antybiotyki.
Summary
Introduction. Bacterial infection of the anal glands has been considered the main cause of anal fistulae for many years. Other most common causes include Crohn’s disease, ulcerative colitis, any type of immunosuppression (e.g. HIV infection, immunosuppressants), foreign bodies, and injuries. Studies assessing the type of bacterial pathogen involved in the formation of an anal fistula are sparse. Furthermore, it seems that although surgery remains the primary treatment of the disease, the importance of treating cryptic infection and the use of antibiotic therapy based on culture findings seems underestimated.
Aim. The aim of this study was to assess the rationale for the use of preventive antibiotic therapy in patients after proctological surgeries.
Material and methods. In the period from January 1 to December 31, 2019, 46 patients (40 men, 6 women) aged 28 to 71 years (mean age 49 years) were operated on at the Department of General Surgery of the County Hospital in Ostrów Mazowiecka for anal fistulae. All patients were operated on by the same surgeon experienced in proctological surgery. Bacterial cultures were collected intraoperatively and preventive antibiotic therapy in the form of IV clindamycin 2 × 600 mg was used in all patients.
Results. A large number of Bacteroides spp. showed high resistance (88%) to clindamycin. Anaerobic bacteria showed 60% resistance to clindamycin.
Conclusions. 1. Clindamycin should not be used in preventive antimicrobial treatment in patients undergoing surgical treatment for anal fistula in the Department of General Surgery of the County Hospital in Ostrów Mazowiecka. 2. The variable sensitivity of bacteria to antimicrobials should be considered and antibiotic prophylaxis should be changed depending on the resistance developed to the subsequent antibiotics used.

Introduction
Bacterial infection of the anal glands has been considered the main cause of anal fistulae for many years. Other causes, which have recently gained importance, primarily include inflammatory bowel diseases such as Crohn’s disease and ulcerative colitis, any type of immunosuppression (e.g. HIV infection, immunosuppressants), foreign bodies and injuries. Studies assessing the type of bacterial pathogen involved in the formation of an anal fistula are sparse. Furthermore, it seems that although surgery remains the primary treatment approach, the importance of treating cryptic infection, e.g. using antibiotic therapy based on culture findings, is underestimated.
One-day antibiotic therapy audits (including Point Prevalence Survey) and perioperative prevention audits have been conducted in the County Hospital in Ostrów Mazowiecka for many years (1). While discussing the results of the audit with the Head of the Department of General Surgery, a decision was made to conduct a study on the rationale for antibiotic therapy (clindamycin) used in patients undergoing proctological procedures. In 2019, samples collected intraoperatively during proctological procedures were delivered to the Laboratory of Diagnostic Microbiology. Microbiological analysis for aerobic and anaerobic bacteria was performed to obtain isolates. Their drug susceptibility and percentage distribution are presented below.
Aim
The aim of this study was to assess the rationale for the use of preventive antibiotic therapy (clindamycin) in patients after surgical treatment of anal fistulae.
Material and methods
In the period from January 1 to December 31, 2019, 46 patients (40 men, 6 women) aged 28 to 71 years (mean age 49 years) were operated on at the Department of General Surgery of the County Hospital in Ostrów Mazowiecka for anal fistulae. All patients were operated on by the same surgeon experienced in performing proctological operations.
Samples (fragments of fistulous tracts) for bacterial culture were collected intraoperatively in all patients.
Preventive antibiotic therapy in the form of clindamycin was used (2).
The research material consisted of 46 anal fistulae, which were used for cultures for aerobic and anaerobic microbes. The aerobic and anaerobic cultures were performed as two separate tests (total positive tests 84 – 80.4% of all delivered fistulas). In order to grow aerobic microorganisms, the material was plated on microbiological media (Columbia agar, MacConkey agar, Sabouraud’s medium with the addition of gentamicin and chloramphenicol, and on a liquid multiplying medium Tryptic Soy Broth). Cultures were incubated for 18-24 hours at 36.7°C. In order to grow anaerobic microorganisms, the material was plated on two-section Scheadler/Scheadler with kanamycin and vancomycin medium and incubated for 48 hours at 36.7°C. Gram-stained direct smear was prepared from each sample, and was assessed microscopically for the presence of bacteria.
Results
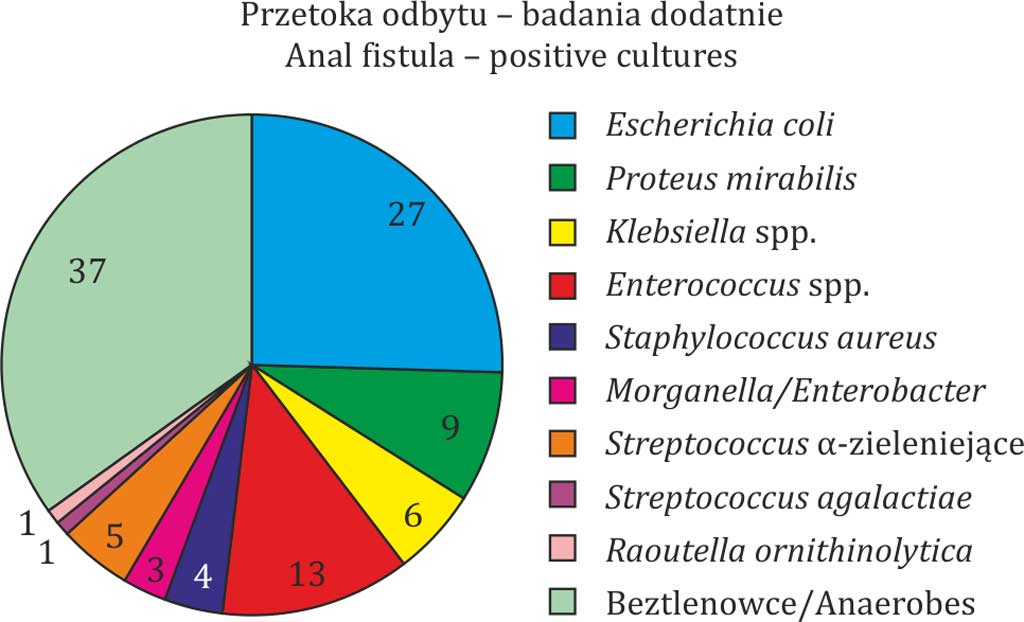
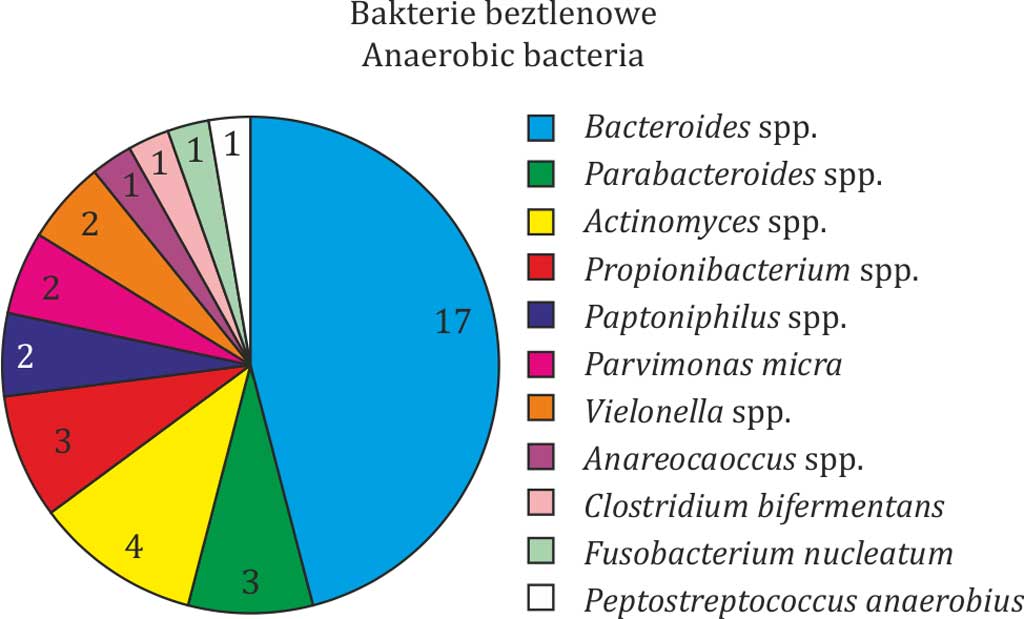
Microbiological analysis of the microorganisms cultured from the samples (fistulas) is shown below (fig. 1, 2).
Fig. 1. Isolates obtained from aerobic and anaerobic cultures
Fig. 2. Isolates obtained from anaerobic cultures
A total of 84 positive cultures (80.4%) were obtained from the analysed samples. Cumulative antibiograms for the most common aerobic and anaerobic microbes were performed. The tables below show the percentage distribution of drug susceptibility of different microbes (tab. 1-5).
I. Aerobic bacteria
In addition to Escherichia coli, Proteus mirabilis, Klebsiella pneumoniae/oxytoca oraz Enterococcus spp., other aerobic, clinically significant bacteria were cultured, for which no collective antibiograms were performed due to single isolations. The following microbes were isolated:
– α-haemolytic Streptococcus – 5 x susceptibility to penicillin,
– Streptococcus anginosus – 1 x,
– Streptococcus parasanguinis – 2 x,
– Streptococcus salivarius – 1 x,
– Streptococcus mitis – 1 x,
– Staphylococcus aureus – 4 x MSSA – susceptibility to beta-lactams.
II. Anaerobic bacteria
In addition to Bacteroides spp., other anaerobic, clinically significant bacteria were cultured, for which a collective antibiogram was performed (tab. 5). The following microbes were isolated:
– Parabacteroides distasonis – 2 x, Parabacteroides merdae – 1 x,
– Actinomyces odontolyticus – 3 x, Actinomyces turicensis – 1 x,
– Propionibacterium granulosum – 2 x, Propionibacterium acnes – 1 x,
– Peptoniphilus asaccharolyticus – 2 x,
– Parvimonas micra – 2 x,
– Veillonella spp. – 2 x,
– Anaerococcus prevotii – 1 x,
– Clostridium bifermentans – 1 x,
– Fusobacterium nucleatum – 1 x,
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Dzierżanowska D: Antybiotykoterapia praktyczna. Wydawnictwo Alfa-Medica Press, Bielsko-Biała 2018.
2. Hryniewicz W, Kulig J, Ozorowski T et al.: NPOA Rekomendacje ,,Stosowanie antybiotyków w profilaktyce okołooperacyjnej”. Warszawa 2011.
3. Seow-Choen F, Hay AJ, Heard S, Phillips RK: Bacteriology of anal fistulae. Br J Surg 1992; 79(1): 27-28.
4. de San Ildefonso Pereira A, Maruri Chimeno A, Facal Alvarez C et al.: Bacteriology of anal fistulae. Rev Esp Enferm Dig 2002; 94(9): 533-536.
5. Sugrue J, Nordenstam J, Abcarian H et al.: Pathogenesis and persistence of cryptoglandular anal fistula: a systematic review. Tech Coloproctol 2017; 21(6): 425-432.
6. Siegmund B, Feakins RM, Barmias G et al.: Results of the Fifth Scientific Workshop of the ECCO (II): Pathophysiology of Perianal Fistulizing Disease. J Crohns Colitis 2016; 10(4): 377-386.