© Borgis - New Medicine 4/2003, s. 82-86
Jolanta Zyczkowska1, Alicja Klich-Raczka1, Barbara Wizner1
Hypertension and cognitive and functional performance in centenarians
1 Department of Internal Medicine and Gerontology, Jagiellonian University Medical College,
Cracow, Poland
Head: prof. Tomasz Grodzicki, MD, PhD
2 International Institute of Molecular Biology, Warsaw, Poland
3 Department of Pathophysiology, University Medical School, Poznan, Poland
Summary
Aim: Assessment of the relationship between hypertension and physical and cognitive performance in centenarians.
Methods: Investigations, performed as a part of the POL STU 99, included 85 participants (12 men and 73 women), aged 100-112 years. We assessed cognitive function with the Mini Mental State Examination (MMSE) based on the 30-points scale, and physical activity with ADL (Activities of Daily Living) test based, on a 12-points scale. Blood pressure was measured 3-6 times on both arms according to the Korotkoff method, in a sitting (if possible) or lying position during one home visit. Hypertension was diagnosed if the average value of the blood pressure exceeded 140/90 mmHg, or if antihypertensive medications were used.
Results: The average age in the group was 101.6 (±1.7) years, the BP average values 148.3 (±24.0)/80 (±11.7) mmHg. Average score of the mental test in the MMSE scale was 16.16 (±10.22), and the average score on the physical test in the ADL scale was 7.6 (±3.67).
Conclusions:
1. Blood pressure in the examined group of centenarians does not reveal any correlation with physical abilities or cognitive performance.
2. Cognitive performance in the group is positively correlated with physical performance.
Table 1. Average ADL score and percentage of hypertension in each of four groups formed of cases with similar MMSE scores.
| MMSE - points | ADL - average value | Hypertension in % |
| 0-9 | 3.7 | 43.5 |
| 10-19 | 7.9 | 68.2 |
| 20-23 | 9.0 | 73.3 |
| ł 24 | 10.1 | 60.0 |
INTRODUCTION
The life expectancy of human beings increases every year. In 1900 the mean length of life in industrialised countries was 46 years, while in 1988 this average had risen to 77 years (1). The past century witnessed a considerable increase in elderly population. Starting in 1960, the number of centenarians living in developed countries is doubling every decade.
Older people, including centenarians are more vulnerable to chronic illnesses, including hypertension and dementia. The prevalence of cognitive impairment is 15% at the age of 65, and increases to 50% at 80 years of age (2).
Cognitive impairment is characterised by the development of intellectual and mental defects, including progressive memory loss, disorientation in space and time, loss of autonomy, and emotional depersonalisation.
Hypertension in the elderly is a well-recognised risk factor for vascular dementia and Alzheimer´s disease. The results of several long-lasting epidemiological studies reveal a positive correlation between hypertension and higher rates of cognitive impairment (3, 4, 5, 6). However, the published data are in consistent (7). Some investigations show no association between dementia and higher blood pressure in elderly subjects (8, 9, 10), studies showing negative correlation (11). The reasons for these apparent discrepancies may be different. Some long-lasting studies compared the midlife BP with late-life cognitive function assessed at a single point in time (3, 4, 5), while in other investigations BP was measured at a single time. Furthermore, the variability of the results may be due to differences in psychological assessment methods, or to the method of selection of the populations investigated. In particular, the total results in an elderly population> 60 years of age are likely to differ from the data obtained for very long-lived people, i.e.> 100 years.
The main goal of this work was to investigate a possible relationship between hypertension, and cognitive and physical impairment in centenarians. This group forms a special sample of the population, for which the following "rule” holds: „the older you get, the healthier you have been” (12).
MATERIAL AND METHODS
This work was conducted as a part of the All Polish Project of Investigations of Polish Centenarians (POLSTU 99), (POLSTU) co-ordinated by the International Institute of Molecular Biology in Warsaw, Poland. The study was performed on subjects born before December 31, 1898, living in the following provinces of central and southeastern Poland: Lubelskie, Lódzkie, Malopolskie, Mazowieckie, Podkarpackie, Śląskie, Świętokrzyskie, and Wielkopolskie. Examinations, performed at the home of each centenarian, consisted of blood pressure measurements and assessments of their mental and physical status, based on home interviews.
Blood pressure was assessed on the basis of several (3-6) measurements using the Korotkoff method, taken on both arms in a sitting (if possible) or lying position at minimum of one minute intervals. Where hypertension was diagnosed, it was based on an average SBP >?140 mmHg or DBP >?90 mmHg, or any current treatment for hypertension.
Mental status was assessed in a 0-30 point scale based on Folstein´s Mini Mental State Examination (MMSE). Scoring was adjusted according to the degree of handicap (e.g. for persons with eye impairment the seeing part of the MMSE test was not taken into account). To describe the mental status of each subject we used the following scale in MMSE points: 0-9 points – severe dementia; 10-19 points – moderate dementia, 20-23 points – mild dementia, 24 points or more – no dementia.
Physical impairment assessment was based on a 12-points ADL scale (ADL – activities of daily living).
RESULTS
We examined 85 individuals, aged 100-112 years, (mean 101.6 ± SD 1.7) (12 men and 73 women).The average systolic, diastolic, and pulse blood pressure were 148.3, 80.0 and 68.3 mm Hg, respectively. Mean MMSE score was 16.2 points, while the mean ADL score was 7.6 points. General characteristics of the study group are provided in Table 2.
Table 2. General characteristics of the examined population.
| | Mean | ?SD | Min | Max |
| Age (years) | 101.6 | 1.7 | 100 | 112 |
| SBP (mm Hg) | 148.3 | 24.0 | 98 | 213 |
| DBP (mm Hg) | 80.0 | 11.7 | 55 | 110 |
| PP (mm Hg) | 68.3 | 19.3 | 36 | 130 |
| MMSE (points) | 16.2 | 10.2 | 0 | 30 |
| ADL (points) | 7.6 | 3.7 | 0 | 12 |
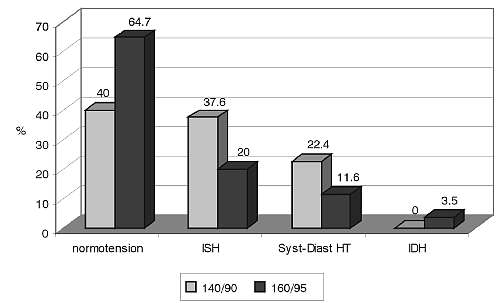
Fig. 1. Hypertension in the analysed group of centenarians.
Figure 1 presents the incidence and type of hypertension in the centenarians. Hypertension, diagnosed as BP of 140/90 mmHg or hypertension treatment, was found in 60 % of individuals. Isolated systolic hypertension (ISH) was diagnosed in 37.6% of the subjects, while systolic/diastolic hypertension was diagnosed in 22.4%. According to a milder, > 160/95 mmHg criterion, the majority of the group (64.7%) were normotensive.
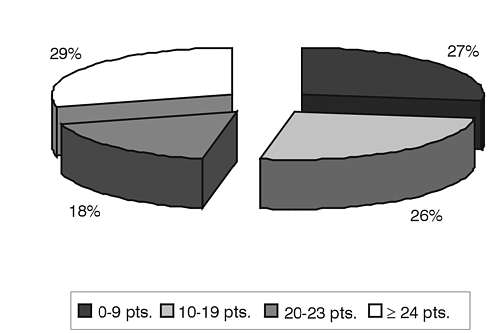
Fig. 2. Cognitive status assessed with MMSE.
The distribution of the MMSE score is illustrated in Fig. 2. The score of almost one-third of the group was very good at > 24 points. On the other hand, 26% scored less than 10, which is a sign of severe dementia.
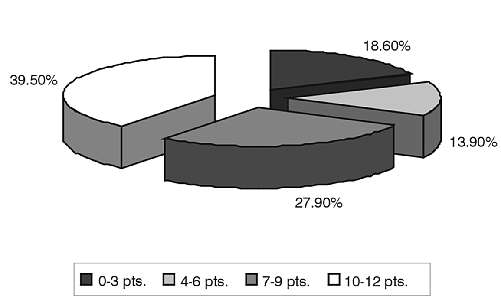
Fig. 3. Physical ability assessed with ADL.
Figure 3 presents the distribution of the ADL score, which characterises physical status. Almost 40% of centenarians scored more than 9 points, signifying their ability to perform the basic activities of daily living (getting up from bed, eating, use of the toilet) by themselves. A much smaller fraction of the analysed group (18.6 %) showed complete functional impairment, reflected by an ADL score of 0-3 points.
Statistical analysis of our data reveals a strong positive correlation between the MMSE score and the physical abilities, assessed by the ADL test – see Fig. 4. The prevalence of hypertension in groups with different grades of dementia is shown in Table 3. In the group of individuals with severe dementia hypertension was diagnosed less frequently than in the remaining group (p = 0.03).
No statistically significant relationship was found between systolic, diastolic, or pulse pressure and the MMSE score.
DISCUSSION
We studied 85 Polish centenarians in order to assess a possible relationship between the frequency of hypertension, cognitive impairment and functional status.
Table 3. Prevalence of hypertension and average ADL score according to MMSE.
|
| Mental impairmentMMSE - points | Physical impairment
ADL - points | Hypertension % (140/90) |
|
a | 0-9 | 3.7 | 43.5 | 43.5* |
|
b | 10-19 | 7.9 | 68.2 | Sb+c+d = 66.1 |
|
c | 20-23 | 9.0 | 73.3 |
|
d | > 24 | 10.1 | 60.0 |
*p=0.03
In the examined group we found 60% of centenarians to be hypertensive according to a SBP > 140 and/or DBP > 90 mmHg criterion or current antihypertensive therapy. This number is slightly higher than the data obtained in the Longitudinal Study of Danish Centenarians, where the prevalence of hypertension was 52%. According to a less restrictive, older criterion – BP >?160/95 mmHg – our results (35.3%) are comparable to Danish (31%) (13). Our study showed a smaller prevalence of hypertension among centenarians (60%) than in younger groups of elderly people, in the Polish population – 81% of women and 66% of men above 64 years of age (14) and 35.3% vs. 65% according to a >?169/95 mmHg criterion (15). The Framingham Heart Study reported the prevalence of hypertension among people aged 75 years and over to be 41% among men, and 54% among women (16). The most frequent form of hypertension observed was isolated systolic hypertension (37.6%), and the same was reported for a group of younger elderly people (15).
It is well-known that the incidence of dementia in the elderly doubles every 5 years. Our findings, that about 70% of centenarians were diagnosed as mildly to severely demented are in accordance with the result from the New England Centenarian Study, where 79% of the 315 subjects demonstrated some degree of cognitive impairment (17). In the Danish study the prevalence of dementia was considerably smaller – 51% among examined centenarians (13). This difference may be due to the fact that the Danish centenarians were a bit younger – all of them ce-lebrated their 100th birthday during the year before the investigation, while in our project there were also older individuals (the oldest woman was 112 and, the oldest man was 104 years old). The differences in outcomes of various studies may be due to the relatively small group sizes and hence large chance variability, and to the fact that the methods of investigation are only adaptations of instruments used in younger individuals. This is true particularly of the MMSE scoring system.
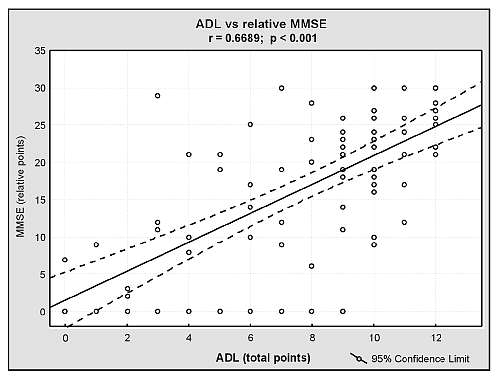
Fig. 4. Correlation between mental and physical ability in the group of centenarians.
Analysing the ADL results obtained in the group of centenarians, we found that 39.5% of them received 10-12 points and were relatively independent, while 32.5% of the group scored less than half the optimal result, which means that they were almost totally dependent upon carers. The results are similar to findings from the Danish study, where the persons categorised as being relatively independent and being totally dependent upon help comprised 41% and 35% of the group (13). In another investigation of centenarians, 35% of the participants were estimated as completely independent (12). It is worth emphasizing that functional impairment, common at the end of their long lives, was uncommon at a mean age of 92 years, when 89% of the individuals were living independently (12).
The relationship between cognitive and functional performance in our project is in agreement with findings from other studies, showing that cognitive impairment in the elderly is usually accompanied by limitations in the activities of daily living (ADL) (18, 19, 20, 21).
Comparing the percentage of hypertension in each of the four groups with the MMSE score, we found that in the subgroup with severe dementia the hypertension (diagnosed according to the 140/90 criterion) occurred significantly less frequently. This observation is consistent with the results of the Danish study, in which hypertension was found to be significantly more frequent in non-demented than in demented participants (22).
Our study does not indicate any correlation between MMSE score and systolic, diastolic, or pulse blood pressure. This observation differs from the results of several other studies. Some studies (Syst Eur Trial, The Honolulu – Asia Ageing Study) confirm a relationship between high systolic blood pressure and lowered levels of cognitive ability (4, 23, 24). Other studies emphasise the relationship between hypertension and dementia (6, 25, 26, 27, 28). The Swedish study (29) indicates that higher pulse pressure is associated with increased risk of Alzheimer´s disease and dementia in the elderly. Moreover, in the same work, a decreased pulse pressure correlated with an increased risk of dementia. However, Glynn et all (25) indicate a non-linear association between blood pressure and cognitive decline (a U – shaped curve), in which the higher as well as the lower pressures were associated with an elevated prevalence of cognitive decline.
On the other hand, some investigations (8, 9, 10) demonstrate no correlation between cognitive function and blood pressure whatsoever.
The apparent discrepancy between our findings and some results published earlier may be due to several factors. First, in the POLStu programme, all centenarians were only examined once, while the majority of the data presented in the quoted papers above were obtained in long-lasting epidemiological investigations. Additionally, our data may be difficult to interpret, since the blood pressure was measured during one day only. Furthermore, a single visit did not allow us to assess the influence of the therapy applied. On the other hand, a long-lasting investigation of people of such an age is hardly possible. Secondly, the vast majority of centenarians enjoyed quite good health during their lives, and started to suffer hypertension or chronic diseases only at their eighties or later (17). Hence a relatively short time, during which they suffered hypertension, has not played a major role in the development of dementia.
In our study the prevalence of hypertension according to the 140/90 criterion was 60%. Most of these however, were stage one hypertensive, as exemplified by a relatively low percentage of persons diagnosed on the 160/95 criterion. On the other hand, our findings may suggest that a moderate increase of blood pressure in very old people may play a role in sustaining adequate circulation in the brain, through more rigid arteries which are less adaptive for autoregulation processes.
Seux et al. emphasise that blood pressure has a smaller influence on cognitive status, in comparison with other factors such as age and education (30).
Our observation, that the prevalence of hypertension decreases with age among an extremely old population, while the percentage of people with cognitive impairment increases with age, may suggest the presence of a blood pressure independent mechanism in the progression of dementia in the oldest group of the population.
CONCLUSIONS
Blood pressure in the group of centenarians does not reveal any correlation with physical abilities or cognitive performance. Cognitive performance in the group correlates positively with physical performance.
Acknowledgements
It gives us great pleasure to thank Dr. J. Gąsowski for reading the manuscript, and for several helpful comments.
Piśmiennictwo
1. GUS: Seniorzy w polskim społeczeństwie. GUS, Warszawa 1999. 2. Abrams W.B. et al.: MSD Podręcznik Geriatrii. Urban & Partner, Wrocław 1999; p 1234. 3. Elias M.F. et al.: Untreated blood pressure level is inversely related to cognitive functioning: the Framingham study. Am. J. Epidemiol. 1993; 138:353-364. 4. Launer L.J. et al.: The association between midlife blood pressure levels and late-life cognitive function: The Honolulu – Asia Ageing Study. Jama; 1995; 274: 1846-1851. 5. Kilander L. et al.: Hypertension is related to cognitive impairment: a 20-year follow-up of 999 men. Hypertension 1998; 31: 780-786. 6. Harrington F. et al.: Cognitive performance in hypertensive and normotensive older subjects. Hypertension 2000; 36: 1079-1082. 7. Seux M.L., Forette F.: Effects of hypertension and its treatment on mental function. Curr. Hypertens. Rep. 1999; 1:232-237. 8. Farmer M., et al.: Longitudinally measured blood pressure, antihypertensive medication use, and cognitive performance: the Framingham study. J. Clin. Epidemiol. 1990; 43:475-480. 9. Scherr P.A. et al.: Relation of blood pressure to cognitive function in the elderly. Am. J. Epidemiol. 1991; 134: 103-1315. 10. Posner H.B. et al.: The relationship of hypertension in the elderly to AD, vascular dementia, and cognitive function. Neurology 2002; 58:1175-1181. 11. Guo Z. et al.: Blood pressure and performance on the Mini-Mental State Examination in the very old. Am. J. Epidemiol. 1997; 145:1106-1113. 12. Hitt R. et al.: Centenarians: the older you get, the healthier you have been. Lancet, 1999, 354:652. 13. Andersen-Ranberg K. et al.: Healthy centenarians do not exist, but autonomous centenarians do: a population – based study of morbidity among Danish centenarians. JAGS 2001; 49:900-908. 14. Kąkol M. et al.: Rozpowszechnienie, świadomość oraz skuteczność leczenia nadciśnienia tętniczego u ludzi starszych w Polsce – ocena metodą sondażu reprezentatywnego. Gerontol. Pol. 1999; 7:(2):23-29. 15. Kocemba J. et al.: Distribution of blood pressure and prevalence of arterial hypertension in the old population of Cracow. Mat. Med. Pol. 1991; I: 33-35. 16. Vokonas P. et al.: Epidemiology and risk of hypertension in the elderly: the Framingham study. J. Hypertens. 1988; 6(suppl. 1):3-9. 17. Evert J. et al.: Morbidity Profiles of Centenarians: Survivors, Delayers, and Escapers. J. Gerontol. Med. Sci. 2003, 58A, 3:232-237. 18. Bidzan L. et al.: Wpływ poziomu funkcji poznawczych i depresji na aktywność złożoną u osób w wieku podeszłym. Gerontol. Pol. 2000, 8 (4):9-14. 19. Tabert M.H. et al.: Functional deficits in patients with mild cognitive impairment. Neurology 2003, 58 (5): 758. 20. Moritz D.J. et al.: Cognitive functioning and the incidence of limitation in activities of daily living in an elderly community sample. Am. J. Epidemiol. 1995, 141, 1:41-49. 21. Boeve B. et al.: Mild cognitive impairment in the oldest old. Neurology 2003; 60, 3:477-80. 22. Andersen-Ranberg K. et al.: Dementia is not inevitable: a population-based study of Danish centenarians. J. Gerontol. B Psychol. Sci. Soc. Sci. 2001; 56, 3: 152-159. 23. Kivipelto M. et al.: Midlife vascular risk factors and Alzheimer´s disease in later life: longitudinal population-based study. BMJ. 2001; 322:1447-1451. 24. Birkenhger W.H. et al.: Blood pressure, cognitive functions, and prevention of dementias in older patients with hypertension. Arch. Intern. Med. 2001; 161:152-156. 25. Glynn R.J. et al.: Current and remote blood pressure and cognitive decline. Jama 1999; 281:438-445. 26. Tzourio C. et al.: Cognitive decline in individuals with high blood pressure: A longitudinal study in the elderly. Neurology 1999; 53:1948-1952. 27. Elias M.F. et al.: Lower cognitive function in the presence of obesity and hypertension: the Framingham heart study. Int. J. Obes. Relat. Metab. Disord. 2003; 27:260-268. 28. Wu C. et al.: Relationship between blood pressure and Alzheimer´s disease in Linxian County, China. Life Sci. 2003; 72: 1125-1133. 29. Qiu C. et al.: Pulse pressure and risk of Alzheimer´s disease in persons aged 75 years and older: a community-based, longitudinal study. Stroke. 2003; 34:594-599. 30. Seux M.L. et al.: Correlates of cognitive status of old patients with isolated systolic hypertension: the Syst-Eur Vascular Dementia Project J. Hypertens. 1998; 16:963-969.
