© Borgis - New Medicine 4/2003, s. 104-107
Krystyna Bogus1,2, Ewa Borowiak1,3, Wojciech Drygas1, Tomasz Kostka1
Comprehensive geriatric assessment of random sample of older inhabitants of Lodz (Poland) – pilot study
1 Department of Social and Preventive Medicine, Medical University of Lodz, Poland
2 Regional Public Health Centre, Lodz
3 Institute of Nursing, Medical University of Lodz
Summary
Aim of the study: To carry out a Comprehensive Geriatric Assessment of a random sample of 200 community-dwelling inhabitants of Lodz above 65 years of age (100 women and 100 men).
Material and methods: Several scales were used: Mini Nutritional Assessment (MNA), Activities of Daily Living (ADL), Instrumental Activities of Daily Living (IADL), Geriatric Depression Scale (GDS), Mini Mental State Examination (MMSE).
Results: The most common illnesses were hypertension (71%), ischaemic heart disease (38.5%) and musculoskeletal disorders (30%). The prevalence of post-myocardial infarction status was almost three times more in men than in women (16 vs 6; p = 0.04). The men smoked four times more than women (18 vs 4; p = 0.0033). Body Mass Index (BMI) values were higher among women (29.2 ± 5.3 vs 26.9 ± 3.9; p = 0.004) as well as the percentage of body fat (44.4 ± 8.0 vs 30.7 ± 4.9; p = 0.001). The men also showed a higher level of ADL functional efficiency (5.88 ± 0.32 vs 5.74 ± 0.41; p = 0.008) and a better nutritional state in the MNA (25.8 ± 2.5 vs 24.8 ± 2.9; p = 0.009). The women were characterised by a higher GDS score (6.10 ± 3.41 vs 4.70 ± 2.98; p = 0.023).
Conclusions: Circulatory and musculoskeletal disorders are the most common health problems found in the group of older inhabitants of Lodz. The men were characterised by almost three times more prevalent post-myocardial infarction status and they smoked four times more than women. The women had more often symptoms of depression, worse nutritional state and lower level of functional efficiency.
INTRODUCTION
The demographic situation is one of the most significant factors influencing both the current and the predicted health situation in Poland and other developed countries (1). In the last 50 years the average length of life in countries with high living standards has risen by 28 years. In Poland more than 16.2% of people reach an age of 60 years. Only 8.8% of these people are healthy, and among the rest the incidence of chronic diseases amounts to 3.8 units per person (2, 3). According to specialists, in the near future in ageing societies, over a half of all patients will be above age 65 (4). The process of life lengthening and the resulting growth in the number of older people requires more attention to the problems and needs of the elderly (5).
Comprehensive Geriatric Assessment (CGA) is a multi-dimensional evaluation used to fully assess the needs of older patients. CGA provides us with information concerning physical and psychological health, and functional efficiency as well as the social and environmental situation of the elderly. It allows the establishment of the extent of health status disorder and medical priorities in older subjects (6, 7).
In Poland, only a few studies have been done on chosen elements of CGA in larger groups of older persons (8, 9, 10). There are no representative studies of different populations of older persons in our country. That is why the aim of this study was to carry out the Comprehensive Geriatric Assessment of a random sample of older inhabitants of Lodz (an industrial city of 800 000 inhabitants).
MATERIAL AND METHODS
The study was carried out in the Gorna district of Lodz during 2002 and 2003. Two hundred persons participated (100 women and 100 men) between 66 and 79 years of age. The respondents were chosen using a proportional poll pattern. All the respondents were community-dwelling elderly. Persons with severe dementia and the terminally ill were excluded from the study. All respondents were informed about the aim of the study and written informed consent was obtained.
The physical examinations were done in the Department of Preventive Medicine, Medical University of Lodz. The rest of each assessment was carried out in the patients´ homes. Information concerning age, gender, education, current and past diseases, medications being taken, and tobacco smoking was obtained. Other elements of the CGA were assessed by different questionnaires. Nutritional state was assessed using the Mini Nutritional Assessment questionnaire (MNA (11). The assessment of the nutritional state was completed by assessing the percentage of body fatty tissue, using the 4 skinfolds method (12), and by measuring the waist to hip ratio (WHR).
Independent living was assessed by the Activities of Daily Living Scale (ADL) (13) and Instrumental Activities of Daily Living (IADL) (14).
To assess the psychological state, the following were used:
a) The Geriatric Depression Scale (GDS). The short version consists of 15 questions, which describe the patient´s well-being. An outcome from 0 to 5 points means no depression characteristics; from 6 to 10 points = moderate depression; from 11 to 15 = severe depression (15)
b) The Mini Mental State Examination (MMSE). In this there are six groups of exercises, which check the level of such basic psychological processes as: time and space orientation, ability to remember and recollect things, concentration and calculation, and language functions. The maximum possible score is 30 points, which shows an overall efficiency in cognitive functions (16).
STATISTICAL ANALYSIS
The one way analysis of variance (ANOVA), chi-square test, and Kruskal-Wallis test were used to analyze the variables. Continuous variables were presented as mean ± standard deviation. The limit of significance was set at p > 0.05.
RESULTS
The average age for the whole group of respondents was 71.53 ± 3.86. The average age of women was comparable to the average age of men (Table 1). The average period of education (years) was similar in both groups. Thirty-six women lived alone, 32 with partner, and 32 women lived with family, while only 9 men lived alone, 70 with partner, and 21 men lived with family (chi-square = 32.6; p <0.001, not shown in the Table). Average family income per capita was classified as high in 26 women, average in 64 women, and low in 10 women. In men, 19 had high income, 78 average, and 3 men had low income (chi-square = 6.24; p = 0.044, not shown in the Table).
The disease incidence in the mens´ and the womens´ groups were comparable with the exception of post-myocardial infarction state, which was more common in men. Also, men smoked four times more often than women. The number of medications taken regularly was similar in both groups. Eye diseases (glaucoma and cataract) and post-stroke status amounted to less than 3% in both groups. The most common illnesses in the older inhabitants of Lodz are presented in Figure 1.
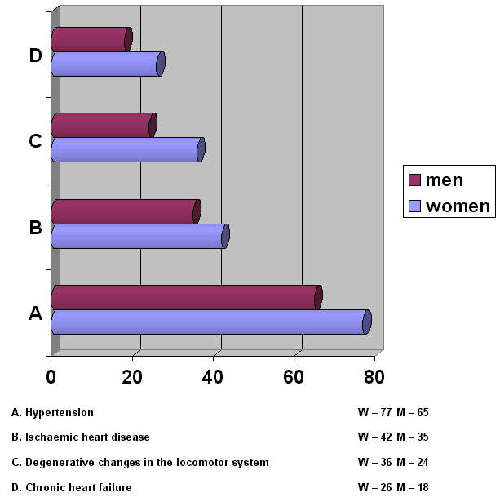
Fig. 1. Chronic health conditions most common in the group of respondents.
The group of women was characterised by a higher BMI and percentage of fatty tissue (Table 1). The waist to hip ratio (WHR) was higher in the men´s group. Also, the significant relationship between nutritional state as assessed by MNA and gender was found. The higher scores were found in the men´s group. Calf circumference was similar in both groups.
The group of women was also showed a lower efficiency in performing basic daily activities (ADL Scale) than men. In IADL similar values were gained in both groups. Women reached higher scores than men in the Geriatric Depression Scale (GDS). The scores in the Mini Mental State Examination (MMSE) were comparable in both groups (Table 1).
Table 1. Comprehensive Geriatric Assessment of random sample of 200 older inhabitants of Lodz.
| | WOMEN (n = 100) | MEN (n = 100) | P - VALUE |
| Age | 71.7 ? 3.9 | 71.4 ? 3.8 | NS |
| Education (years) | 9.5 ? 3.2 | 9.7 ? 3.5 | NS |
| Ischaemic heart disease (%) | 42 | 35 | NS |
| Respiratory diseases (%) | 5 | 5 | NS |
| Musculoskeletal disorders (%) | 36 | 24 | NS |
| Stomach/duodenal ulceration (%) | 4 | 4 | NS |
| Diabetes (%) | 15 | 19 | NS |
| Hypertension (%) | 77 | 65 | NS |
| Chronic heart failure (%) | 26 | 18 | NS |
| Post myocardial infarction (%) | 6 | 16 | p = 0.04** |
| Smokers (%) | 4 | 18 | p = 0.0033** |
| No. of medications taken regularly | 3.8 ? 2.6 | 3.2 ? 2.4 | NS |
| BMI (kg/m2) | 29.1 ? 5.3 | 26.9 ? 3.9 | p = 0.004*** |
| WHR | 0.83 ? 0.05 | 0.94 ? 0.07 | p < 0.001* |
| Body fat (%) | 44.4 ? 8.0 | 30.7 ? 4.9 | p = 0.001* |
| Calf circumference (cm) | 36.9 ? 5.0 | 37.4 ? 3.9 | NS |
| MNA | 24.8 ? 2.9 | 25.8 ? 2.5 | p = 0.009*** |
| ADL | 5.7 ? 0.4 | 5.9 ? 0.3 | p = 0.008* |
| IADL | 7.5 ? 1.0 | 7.4 ? 1.3 | NS |
| GDS | 6.1 ? 3.4 | 4.7 ? 3.0 | p = 0.023* |
| MMSE | 26.5 ? 3.8 | 27.0 ? 2.9 | NS |
* = ANOVA; ** = chi-square test; * * * = Kruskal-Wallis test; NS = non signi
DISCUSSION
Comprehensive Geriatric Assessment has become the basis of modern geriatrics, enabling planning of therapy and possible preventive measures. In this study CGA was carried out at random sample of older inhabitants of Lodz. Numerous validated questionnaires and scales were used in order to assess different health and functional aspects. The results are generally similar to those presented in national and foreign studies, which deal with the Comprehensive Geriatric Assessment of the elderly, and use different screening tools (5, 9, 17).
In assessing the health state of the elderly, it is important to take into consideration the incidence of chronic diseases. The most important are the diseases which influence the patient´s efficiency in performing daily activities such as: locomotor system diseases, ischaemic heart disease, chronic heart failure, hypertension, chronic respiratory insufficiency, and sight and hearing impairment.
The incidence of hypertension increases with advancing age. This tendency is stronger in the case of older women (18). In this study, hypertension was detected in 142 subjects (71% of all the respondents in the study). Ischaemic heart disease most often occurs between the ages of 55 and 65, but 55% of all patients suffering from myocardial infarction are aged more than 65, and 80% of deaths resulting from this disease concern patients over 65 years (6). In our groups of respondents there were 77 persons with ischaemic heart disease (38.5%) and 22 persons with post-myocardial infarction status (11%). Therefore, hypertension and ischaemic heart disease are of the highest significance in the polipathology of the elderly in the study. Forty-four subjects (22%) suffered from chronic heart failure. In an earlier bibliography it was reported that 5% of people aged 65-75 years, and 10-20% of people aged 80 years suffer from this disease (19). However, these results seem to be underestimated – chronic heart failure has been diagnosed in 53% of patients aged more than 65, seeking medical help at outpatient clinics for any cause (Rywik 2002). Diabetes affects approximately 20% of the elderly (21). In this study there were 34 subjects (17%) with diabetes. As predicted, musculoskeletal disorders were next to heart and blood vessel diseases as the most common health problems of older individuals (30%).
Functional efficiency in performing basic daily activities was similar to that of residents in retirement homes in the USA – 5.6 vs 5.8 (22). The maximum score, 6 points, was achieved by 74% of respondents. In analogous studies carried out among residents of nursing homes in Lodz, 54% of subjects got 6 points (23). In assessing the extent of depression, our respondents achieved lower scores comparing to analogous studies – 5.5 vs 6.4 (24). The mean score in the Mini Mental State Examination (MMSE) in our group of respondents was 26.8 points. Similar results were obtained during an examination of the older inhabitants of Poznan – 27.7 points (25).
As in previous reports, the credibility of the results in this study is undoubtedly influenced by sampling methodology. Although CGA was carried out at random sample of older inhabitants, our respondents were sufficiently physically fit and independent, as well as mentally healthy, to come to our outpatient clinic and respond to several questionnaires. This sample, therefore, does not fully reflect the real conditions and general state of health of the elderly population. Also, in this study, we assessed mainly health state and functional efficiency. To a lesser extent, the study dealt with the assessment of social and environmental factors.
To sum up, the study proved that the most common diseases among the older inhabitants of Lodz are hypertension, ischaemic heart disease, and degenerative changes in the locomotor system. Post-myocardial infarction status was almost three times more often detected in men, who also smoked four times more often than women. Women showed depressive characteristics more often than men, and a lower functional efficiency in performing basic daily activities. These data should be helpful in improving the detection and understanding of the needs of older persons.
CONCLUSIONS
1. Hypertension, ischaemic heart disease, and musculoskeletal disorders were the most common diseases in the random sample of older inhabitants of Lodz.
2. Post-myocardial infarction status was almost three times more prevalent in men, and their smoking frequency was almost four times that in women.
3. Women showed depressive characteristics more often than men, and were characterised by a lower functional efficiency in performing basic daily activities.
Piśmiennictwo
1. Nowak L.: Sytuacja demograficzna ludzi starszych w Polsce w perspektywie do 2010 roku. Gerontologia 2001. 2. Jabłoński L., Wysokinska-Miszczuk J.: Podstawy gerontologii i wybrane zagadnienia z geriatrii. Wydawnictwo Czelej, Lublin, 2000. 3. Kucharska-Ciesielska M., Marciniak G.: Seniorzy w polskim społeczeństwie. GUS, Warszawa 1999. 4. Szukalski P.: Najstarsi Polacy: szkic demograficzny. Gerontologia Polska 2000; 8(4):3-8. 5. Bień B.: Społeczno środowiskowe uwarunkowania starzenia się populacji. Zdrowie Publiczne 1997; (CVII), 10:273. 6. Kocemba J., Grodzicki T.: Zarys Gerontologii Klinicznej. Medyczne Centrum Kształcenia Podyplomowego Uniwersytetu Jagiellońskiego, Kraków 2000; 35. 7. Abrams W.B. i wsp.: MSD Podręcznik geriatrii. Urban & Partner; Wrocław 1999. 8. Bień B. i wsp.: Kwestionariusz EASY-Care: założenia i metodologia badań. Gerontologia Polska 1999; 7(2): 37-41. 9. Miller M., Gębka Kuczerowska A.: Ocena stanu Zdrowia ludzi w starszym wieku w Polsce. Gerontologia Polska 1988; 6(3-4):18-23. 10. Wojszel B. i wsp.: Kwestionariusz EASY-Care jako system oceny ludzi starszych w praktyce lecznictwa podstawowego. Gerontologia Polska 2000; 8(4):49-53. 11. Guigoz Y. et al.: Mini Nutritional Assessment: a practical assesment tool for grading the nutritional state of elderly patients. Facts and Research in Gerontology 1994; 2: 15-59. 12. Durnin J.V., Womersley J.: Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br. J. Nutr. 1974; 32:77-79. 13. Katz S. et al.: Studies of illness in the aged: The index of ADL, a standardised measure of biological and psychosocial function. JAMA 1963; 185:914-919. 14. Lawton M., Brody E.: Instrumental Activities of Daily Living (IADL) Scale: Orginal observer-rated version. Psychopharmacol. Bull. 1988; 24:785-792. 15. Yesavage J.A. et al.: Development and validation of a geriatric depression screening scale: a preliminary report. J. Psychiatr. Res. 1983; 17:37-49. 16. Folstein M.F. et al.: „Mini-Mental State”: a practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975; 12:189-198. 17. Szwarc H., Szyszko-Wydra B.: Ocena własnego życia, a aktualna sytuacja psychospołeczna badanych osób starszych. Gerontologia Polska 1999; 7(1):33-37. 18. Grodzicki T., Kocemba J.: Nadciśnienie tętnicze u osób w podeszłym wieku. Via media. Gdańsk 2000. 19. Baron T., Gryglewska B.: Rozkurczowa niewydolność serca – patogeneza i implikacje terapeutyczne. Terapia 2002; 12(131):6-15. 20. Rywik S.L. et al.: Heart failure in patients seeking medical help at outpatients clinics. Part I. General characteristics. Eur. J. Heart Fail. 2000; 2(4):413-421. 21. Ornowska-Kunikowska E., Semetkowska-Jurkiewicz E.: Cukrzyca w wieku podeszłym. Terapia 2002; 12(131):16-18. 22. Winograd C.H. et al.: Development of a physical performance and mobility examination. J. Am. Geriatr. Soc. 1994; 42: 743-749. 23. Borowiak E., Kostka T.: Ocena sprawności funkcjonalnej osób starszych na podstawie badań przeprowadzonych wśród mieszkańców Łodzi. Materiały seminaryjne VI Seminarium CINDI WHO – Łódź 2002; 264-272. 24. Gruszeczka D. i wsp.: Socjomedyczne uwarunkowania stanu emocjonalnego pacjenta geriatrycznego podczas hospitalizacji. Gerontologia polska 1998; 6(2):46-51. 25. Jóźwiak A. i wsp.: Zaburzenia pamięci u osób starszych oceniane testem Mini Mental Scale (MMS). Gerontologia Polska 2000; 8(1):46-50.
Pozostałe artykuły z numeru 4/2003:
