© Borgis - New Medicine 4/2009, s. 85-88
Lechosław P. Chmielik, *Magdalena Fršckiewicz, Mieczysław Chmielik
DIAGNOSTIC AND THERAPEUTIC DIFFICULTIES IN CASES OF FOREIGN BODY IN THE OESOPHAGUS IN CHILDREN TREATED IN THE PAEDIATRIC ENT CLINIC WUM IN 2005-2009. CASE REPORTS
Department of Paediatric Otorhinolaryngology, Medical University of Warsaw, Poland
Head of Department: Prof. Mieczysław Chmielik, MD, PhD
Summary
Foreign body in the oesophagus is a problem that may present many difficulties, both diagnostic and therapeutic. A retained foreign body in the oesophagus can cause many severe systemic complications.
Aim. Analysis of diagnostic and therapeutic proceedings in foreign body cases in children treated in the Paediatric ENT Clinic WUM.
Material. Children with a foreign body in the oesophagus treated in the Paediatric ENT Clinic WUM between January 2005 and June 2009.
Results. The authors analyzed diagnostic procedures and results of treatment regarding children with a foreign body in the oesophagus treated in the Paediatric ENT Clinic WUM.
Conclusions. 1. Every case of foreign body in the oesophagus should be verified by endoscopic methods. 2. Long-term retention of a foreign body in the oesophagus can cause serious consequences for the patient´s health and life. 3. In every case of foreign body in the oesophagus posterior-anterior and lateral chest X-ray should be carried out. 4. In cases of small non-radiopaque foreign bodies, radiogram of the oesophagus with cotton is necessary. 5. In children foreign body in the oesophagus can be a result of an unfortunate accident or criminal actions. 6. An extremely dangerous foreign body in the oesophagus is a button-type battery.
INTRODUCTION
Ingestion of foreign bodies among children is common (1) and is a problem that may present many difficulties, both diagnostic and therapeutic. Foreign bodies reach the oesophagus by accident, because of inattention during playing. They include coins, small toys, parts of toys, buttons and batteries. They can also be food elements, e.g. hard food pieces, animal bones and fish bones. It can also happen that the foreign body in the child´s oesophagus is a result of criminal actions (fig. 1).

Fig. 1. Cotton swabs removed from the oesophagus of a 10-day-old infant.
Retained foreign bodies in the oesophagus are located mostly in anatomical narrowings, as follows (2):
– most frequently – narrowing I (oesophagus mouth) in 44.3%
– between narrowings I and II in 28.1%
– narrowing II (crossing of aorta and bronchus) in 19%
– between narrowings II and III in 6%
– narrowing III (hiatus of diaphragm) in 2.5%
Symptoms of foreign bodies in the oesophagus include difficulties in swallowing, odynophagia, vomiting, and sialorrhoea (2, 5, 6).
In diagnostics we should use radiogram of neck, chest and abdomen (exclusion of perforation), radiogram of oesophagus with barite or cotton, computed tomography, and endoscopic examination (2, 6).
To remove a foreign body from the oesophagus we perform the following procedures: rigid oesophagoscopy and surgical removal in cases of extensive bleeding if the foreign body is penetrating the oesophageal wall or cannot be otherwise removed (2, 5).
Complications resulting from the foreign body can be divided into two groups: early complications include ulceration, inflammation of the oesophageal wall, perforation, inflammation of the mediastinum, injury of the aorta, and respiratory distress (1, 2, 3, 4, 5); long-term complications include tracheoesophageal fistula, oesophageal fistulas, and oesophageal stenosis (2, 5).
AIM
Analysis of diagnostic and therapeutic procedures of foreign body cases in children treated in the Paediatric ENT Clinic WUM between 2005 and 2009.
MATERIAL AND METHODS
In the period from January 2005 to June 2009, 45 children with foreign body in the oesophagus, 17 boys and 28 girls with medium age 3 years and 11 months (the youngest 10 days, the oldest 14 years and 5 months) were hospitalized in the Paediatric ENT Clinic WUM.
RESULTS
Among analyzed patients 28 cases of foreign body in the oesophagus were confirmed. No foreign body was found in 10 cases. Foreign bodies in distal parts of the alimentary tract were found in 6 cases. A foreign body was vomited in one case during hospitalization.
Table 1. Kind of removed foreign body.
| Kind of foreign body | Number of cases |
| Coin | 20 |
| Jewellery (earring, ring, pendant) | 3 |
| Part of toy | 2 |
| Battery | 2 |
| Button | 2 |
| Hair-pin | 1 |
| Bone | 1 |
| Wasp | 1 |
| Pill | 1 |
| Needle | 1 |
| Cotton swabs (9 pieces) | 1 |
The following complications of foreign body retention in the oesophagus were observed:
– concentric burn of oesophageal wall at site of battery´s retention – child transferred to the surgical ward,
– granulation at site of foreign body´s retention – 2 cases,
– bed-sore at site of foreign body´s retention – 4 cases,
– injury of mucosa – 5 cases.
Medium period of hospitalization was 2 days.
Table 2. Location of foreign body in the oesophagus.
| Location of foreign body | Percentage of cases (%) |
| narrowing I (oesophagus mouth) | 25 |
| between narrowings I and II | 29 |
| narrowing II (crossing of aorta and bronchus) | 25 |
| between narrowings II and III | 8 |
| narrowing III (diaphragm hiatus) | 8 |
Case # 1
A 2-year-old girl was admitted to the hospital because of sialorrhoea and vomiting after ingesting a metal pendant (scorpion-like). During examination she was anxious, without dyspnoea; in the oral cavity and pharynx retention of saliva was noted; vesicular respiration was normal. In the chest X-ray a radiopaque foreign body in the cervical part of the oesophagus was confirmed. The foreign body (a metal scorpion-shape pendant) was removed during rigid oesophagoscopy with forceps from the second oesophageal narrowing under general anaesthesia. Injury of mucosa of anterior-lateral and posterior oesophageal wall was observed. Dexaven and Augmentin were administered intravenously. The child stayed on empty stomach. On the first day after the procedure a control chest X-ray was done – the result was normal; liquid diet was introduced then pasty diet; no disorders of swallowing were observed. She was discharged in a good condition on the second day after oesophagoscopy (fig. 2, 2a).
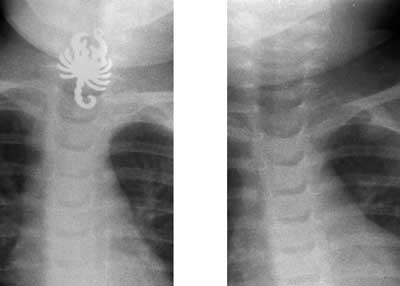
Fig 2, 2a. Chest X-ray before and after removal of foreign body (metal pendant).
Case # 2
A 2-year-old girl ingested a button battery. The parents came to the Hospital in Sokołów Podlaski because the child presented choking. Chest X-ray was done and a round, radiopaque foreign body in the oesophagus was confirmed. The child was transported to the Paediatric ENT Clinic in Warsaw. A button battery was removed during rigid oesophagoscopy under general anaesthesia; in the place of battery retention a mucosal burn was observed. A stomach tube was left; oral feeding was restrained; Augmentin and Dexaven were administered. On the 3rd day after the procedure the girl was transferred to the Paediatric Surgery Clinic, where parenteral nutrition was introduced. On the 4th day fever appeared, blood tests and blood culture were taken, high parameters of inflammatory state were noted, and Augmentin was changed for Fortum and Netromicin. A central insertion for parenteral nutrition was set up. During the following days there was no fever. Gradually Dexaven was discontinued, and Pulmicort Turbuhaler was administered. On the 14th day Netromicin was discontinued. On the 15th day Fortum and Dexaven were discontinued, and oral feeding was started. On the 19th day of hospitalization she was discharged home in a good condition. A control barium swallow was planned in a 2-week-period (fig. 3).

Fig. 3. Chest X-ray of oesophagus with a button battery.
Case # 3
A 2-year-old boy was admitted to the hospital because of vomiting after ingesting solid food. Symptoms had been present for a week. A week earlier he was hospitalized in a different medical centre with a suspected foreign body of the oesophagus for three days. Chest X-ray, which was normal, was performed; after observation the child was discharged. After admission to our hospital chest X-ray was performed; no radiological signs of foreign body were noted. Then radiogram of the oesophagus with barite was performed, in which widening of the upper part of the oesophagus and content retention were noted. The next day under general anaesthesia a foreign body (button) was removed during rigid oesophagoscopy with forceps; it was located below the first oesophageal narrowing. Bed-sore of mucosa at the site of foreign body retention was observed. He was discharged in a good condition on the first day after oesophagoscopy.
DISCUSSION
Foreign body ingestion is common among children. However, this condition may present many difficulties, both diagnostic and therapeutic. Small children have easy access to miniaturized electronic equipment and fancy toys with very small elements; when left unattended they can easily ingest a foreign body. In our study coins were the most frequent foreign bodies found in the oesophagus of children. Literature reports that the most frequent location of a foreign body is in the first narrowing (oesophagus mouth) (2) but we in this study found foreign bodies most frequently between the first and second narrowing, and in second position in the first and second narrowing (both 25%). An extremely dangerous foreign body in the oesophagus is a button battery. Ingestion of a button battery may lead to very severe complications, occasionally even including mortality (7). The risk of complications is determined by the site of the battery´s retention, the duration it remains in the alimentary tract and the possibility of heavy metal absorption (8). Complications of the battery´s retention are caused by a combination of four mechanisms: leakage of alkali causing direct caustic injury, absorption of toxic substances, pressure necrosis and electrical discharge, producing mucosal burns (8). The management with a patient with button battery ingestion depends on the complications. In case of oesophageal burns without perforation a stomach tube, parenteral feeding, steroids and antibiotics should be instituted (9). In the case of our patient such management led to total recovery. In more severe complications, such as oesophageal perforation and mediastinal leakage, thoracotomy is needed. In case of button battery ingestion early recognition is very important; the shape of the battery in chest radiograms is similar to a coin. These patients should be referred to centres competent to deal with such complicated problems.
CONCLUSIONS
1. Every case of foreign body in the oesophagus should be verified by endoscopic methods.
2. Long-term retention of a foreign body in the oesophagus can cause serious consequences for the patient´s health and life.
3. In every case of foreign body in the oesophagus posterior-anterior and lateral chest X-ray should be performed.
4. In case of small non-radiopaque foreign bodies radiogram of the oesophagus with cotton is necessary.
5. In children foreign body in the oesophagus can be a result of an unfortunate accident or criminal actions.
6. An extremely dangerous foreign body in the oesophagus is a button-type battery.
Piśmiennictwo
1. Bhayani MK, Smith AD, Baroody FM et al.: Distal esophageal foreign bodies: Is it a common occurrence post-fundoplication requiring immediate intervention? Inter J of Ped Otorhinolaryngol 2009; 73: 377-81. 2. Otolaryngologia Dziecięca (red.) D. Gryczyńskiej, 2007. 3. Waltzman ML, Baskin M, Wypij D et al.: A randomized clinical trial of the management of esophageal coins in children. Pediatrics 2005; 116(3): 614-9. 4. Soprano JV, Mandl KD: Four strategies for the management of esophageal coins in children. Pediatrics 2000; 105(1): 1-5. 5. Otorynolaryngologia praktyczna (red.) G. Janczewskiego, 2005. 6. Bluestone, Stool, Alper et al.: Pediatric Otorynolaryngology. 7. Hamilton JM, Schraff SA, Notrica DM: Severe injuries from coin cell battery ingestions: 2 case reports. 8. Samad L, Ali M, Ramzi H: Button battery ingestion: hazards of esophageal impaction. J Pediatr Surg 1999; 34: 1527-31. 9. Kost KM, Shapiro RS: Button battery ingestion: A case report and review of literature. J Otolaryngol 1987; 16: 252-7. 10. Al-Qudah A, Daradkeh S, Abu-Khalaf M: Esophageal foreign body. Eur J Cardiothorac Surg 1998 May; 13(5): 494-8.
