© Borgis - New Medicine 4/2009, s. 89-91
*Lechosław P. Chmielik
FOREIGN BODIES IN THE NOSE, THROAT, OESOPHAGUS, TRACHEA AND BRONCHI IN CHILDREN
Department of Paediatric Otorhinolaryngology, Medical University of Warsaw, Poland
Head of Department: Prof. Mieczysław Chmielik, MD, PhD
Summary
The GP or paediatrician often has to deal with foreign bodies in the nose, throat, oesophagus, trachea and bronchi in children. Foreign bodies can be lacerating, swelling, biologically aggressive or of button type. Such batteries are no longer hermetic after a few hours, and their caustic contents cause necrosis in the surrounding tissues. If the battery gets stuck in the oesophagus the result can be life-threatening mediastinitis or even bleeding from the closely-located aorta or pulmonary arteries. Removal of foreign bodies in children from the nose, ear, respiratory tract and oesophagus is described. A foreign body located in the lower respiratory tract may endanger a child´s life by possible asphyxiation. Therefore, prevention is of particular importance. This means that the child must be protected from taking into its mouth objects whose shape and size may cause the danger of aspiration into the lower respiratory tract. Special attention should be paid to toys whose small elements can easily separate from the whole and pose the above-mentioned threat. Typical anamnesis in the case of aspiration of a foreign body into the lower respiratory tract is a paroxysmal cough connected with cyanosis of the patient.
A flexible bronchoscope must not be used to remove foreign bodies from the lower respiratory tract. Such an attempt may easily end up in asphyxiation of the patient. The only instrument to be used is a rigid bronchoscope.
A child, especially a young child, examines the surrounding world with all the senses, including the sense of taste. So, the child will put various objects into the mouth. This may end up in swallowing or aspiration. There are also children who will put small objects into their nose or ears. Such a situation requires a doctor´s intervention, since it may turn into a serious illness or even result in the death of the patient.
The GP or paediatrician often has to deal with this problem. The risk connected with a foreign body finding itself in the patient´s internal organs depends on the kind of object and its location.

Fig. 1. Hard, smooth foreign bodies.
Hard, smooth foreign bodies
Hard, smooth foreign bodies may be difficult to remove because the tool required, for example forceps, may fail to grasp the object.
Lacerating foreign bodies
If the foreign body has cutting edges or any protruding hook-like elements, it may, while being removed, damage surrounding tissues, which especially in the oesophagus or trachea may cause dangerous injury to the adjacent organs (aorta, pulmonary arteries, mediastinum).
Swelling foreign bodies
Another danger can be caused by swelling foreign bodies which are easily inserted into the nose or the external auditory canals. Having swollen, they wedge in the bones and sometimes require surgical intervention, i.e. removal of those bones (1).
Biologically aggressive foreign bodies
The objects in question are often food articles such as peas and beans (and therefore easily available) which often go into children´s noses and ears.
Nuts (mainly walnuts) are most commonly extracted from the lower respiratory tract. They are biologically aggressive. It is not quite clear why these particular objects find their way there. The danger here is blockage of the passage of air through the larynx and trachea. This can be followed by pulmonary abscess, resulting from a local inflammatory reaction caused by thin fragments of the nuts wedged in the small bronchi.

Fig. 2. Hard, cutting foreign bodies.

Fig. 3. Swelling organic foreign bodies.

Fig. 4. Biologically aggressive foreign body.
Button type battery
A particularly dangerous foreign body finding its way into the child´s internal organs is a button type battery. Such batteries are no longer hermetic after a few hours, and their caustic contents cause necrosis in the surrounding tissues. If the battery gets stuck in the oesophagus the result can be life-threatening mediastinitis or even bleeding from the closely located aorta or pulmonary arteries.
The same battery in the stomach may cause a perforation of its wall and an often fatal peritonitis. This kind of battery located in the nose may lead to extensive necrosis of the surrounding tissues and damage of the contents of the orbital and anterior fossa of the skull (2).

Fig. 5. Button type battery.
Removal of foreign bodies from the nose in a child
The best instrument to remove foreign bodies from a child´s nose is a hook.
The hook must be passed over the foreign body and then lowered to complete the removal. If the foreign body stays in the nose for a long period it can be enveloped in granulation. This may hamper its localization and removal, with the additional problem of bleeding. Good orientation in this area is extremely important because adjacent areas contain the anterior fossa of the skull as well as the optic nerve at the medial wall of the orbit. General anaesthesia is required for small children (2, 3).

Fig. 6. A hook for removing foreign bodies.
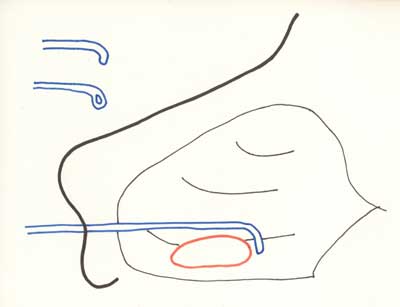
Fig. 7. The way to remove a foreign body from the cavum nasi using a hook.
Removal of foreign bodies from the external auditory canal
As in the case of foreign bodies in the nose, a hook can be used to remove foreign bodies from the external auditory canal. Extreme care should be taken, however, not to push the foreign body towards the tympanic membrane as it may cause luxation of the ossicula with resulting hypoacusis. A much safer way is syringing of the ear. A strong stream of water is directed against the posterior and superior walls of the external auditory canal. To go ahead with the syringing we must be absolutely sure that the tympanic membrane is not perforated. Without this certainty the syringing must not be administered. Especially dangerous are swelling foreign bodies – if they are not removed quickly they will increase their volume and wedge up in the osseous walls of the ear. Their removal is then only possible by surgical widening of the external auditory canal. In the case of small or restive children general anaesthesia should be applied to ensure safe removal (4).
Foreign bodies in the larynx, trachea and bronchi
A foreign body located in the lower respiratory tract may endanger a child´s life by possible asphyxiation (5). Therefore, prevention is of particular importance. This means that the child must be protected from taking into its mouth objects whose shape and size may cause the danger of aspiration into the lower respiratory tract (6). Special attention should be paid to toys whose small elements can easily separate from the whole and pose the above-mentioned threat. Typical anamnesis in the case of aspiration of a foreign body into the lower respiratory tract is a paroxysmal cough connected with cyanosis of the patient (7, 10).
Unless the conditions lead to asphyxiation the symptoms will soon go away. The coughing returns in its paroxysmal form. A foreign body unremoved for a period of several days may cause untreatable pneumonia, local atelectasis or, in extreme cases, valve emphysema. Such symptoms provide an indication for a radiological examination of the thorax (8). Sometimes the x-ray examination fails to confirm the existing condition. Therefore the anamnesis starting the paroxysmal cough is often sufficient to send the child for bronchoscopy. This is the only sure method to confirm or deny the existence of the foreign body (9).
Let me point out categorically that a flexible bronchoscope must not be used to remove foreign bodies from the lower respiratory tract. Such an attempt may easily end up in asphyxiation of the patient (11-20). The only instrument to be used is a rigid bronchoscope.
Piśmiennictwo
1. Sih T, Chinski A, Eavey R (red.): II Manual of Pediatric Otorhinolaryngology IAPO/IFOS 2001: 46. 2. Chmielik M (red.): Schorzenia otolaryngologiczne u dzieci. 2008; 85-86. 3. Chmielik M: Ciała obce w jamie nosogardłowej. Pol. Tyg. Lek. 1073; 28: 1693-1694. 4. Becker W, Naumann HH, Pfaltz CR (red.): Ear, Nose and Throat Diseases. 1994: 77-78. 5. Shubha AM, Kunishka D: Tracheobronchial foreign bodies in infants. I J Ped. Otorhinolar. 2009; 73: 1385-1389. 6. Kubicka K, Kawalec W (red.): Pediatria 2006; 235-236. 7. Becker W, Naumann HH, Pfaltz CR (red.): Ear, Nose and Throat Diseases 1994; 414. 8. Black RE, Matlak ME, Johnson PG: Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surgery 1994: 29; 682-684. 9. Heger CM, Bollmeier ME, Rossler L et al.: Evaluation of clinical radiological and laboratory prebronchoscopy findings in children with suspected foreign body aspiration. J. Pediatr. Surg. 2006; 41: 1882-1888. 10. Bluestone CD, Stool SE, Alper CM et al.: (red.): Pediatric Otolaryngology 2003: 1384. 11. Zawadzka-Głos L, Jakubowska A, Zajšc B et al.: Foreign bodies in the airways in children. New Medicine 2001; 2: 20-22. 12. Zaytoun GM, Rouadi PW, Baki DH: Endoscopic management of foreign bodies in the tracheobronchial tree: predictive factors for complications. Otolaryngol. Head. Neck. Surg. 2000 Sep; 123(3): 311-16. 13. Barben J, Berkowitz RG, Kemp A et al.: Bronchial granuloma – where is the foreign body? Int. J. Pediatr. Otorhinolaryngol. 2000 Jul; 14: 53(93): 215-19. 14. Pirożyński M: Bronchofiberoskopia. Medica Press 1999. 15. Skoulakis CE, Doxas PG, Papadakis CE et al.: Bronchoscopy for foreign body removal in children. A review and analysis of 210 cases. Int. J. Pediatr. Otorhinolaryngol. 2000 Jun; 30: 53(2): 143-8. 16. Shapiro NL, Kaselonis GL: Tracheobronchial foreign body management in an acutely ill neonate. Int. J. Pediatr. Otorhinolaryngol. 2000 Jan 30; 52(1): 75-7. 17. Oguz F, Citak A, Unuvar E et al.: Airway foreign bodies in childhood. Int. J. Pediatr. Otorhinolaryngol. 2000 Jan 30; 52(1): 11-16. 18. Tan HK, Brown K, McGill T et al.: Airway foreign bodies (FB): a 10-year review. Int. J. Pediatr. Otorhinolaryngol. 2000 Dec 1; 56(2): 91-99. 19. Baharloo V, Veyckemans F, Francis C et al.: Tracheobronchial foreign bodies: presentation and management in children and adults. Chest 1999 May; 115(5): 1357-62. 20. Samad L, Ali M, Ramzi H: Tracheobronchial foreign body aspirations in childhood: a 10-year experience. Eur. J. Cardiothorac. Surg. 1998 Oct; 14(4): 388-92.
