© Borgis - New Medicine 2/2013, s. 44-46
*Konrad Wroński1, 2
Surgical treatment giant spermatic cord lipoma – case report
1Department of Oncology, Faculty of Medicine, University of Warmia and Mazury in Olsztyn, Poland
Head of Department: prof. Sergiusz Nawrocki, MD, PhD
2Department of Surgical Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department: Andrzej Lachowski, MD
Summary
Lipoma is the most common benign neoplasm in the human body but frequent under-diagnosed and ignored due to its benign character. The term “giant lipoma” is used for tumors whose size exceeds 10 cm. The author present the rare case of a giant spermatic cord lipoma that was referred as a right inguinal hernia.
INTRODUCTION
Lipoma is the most common benign neoplasm in the human body which develops from the adipose tissue. These tumors are under-diagnosed and ignored by doctors because its benign character. Lipomas are the most frequent found in middle age and in the male population. Many lipomas are small with diameters of about 1-3 cm. The term “giant lipoma” is used for tumors whose size exceeds 10 cm.
The author of this article report the rare case of a giant spermatic cord lipoma that was referred as a right inguinal hernia and found in PubMed Database several articles relating to that described problem (1, 2).
CASE REPORT
A 52-year-old white man referred to the department due to a giant tumor on the right side of the inguinal area. The tumor had been steadily increased in size from 43 months. The patient has reported pain in this region. He had no any other symptoms, such as bowel- or urinary-altered habitus, previous surgeries, previous hospital admission or drug abuse.
On physical examination, in the right inguinal area a giant tumor was palpable. The size of the tumor during examination was 14 x 8 cm (fig. 1). Testicles were painless and normal in size and consistency. The abdominal examination was also normal.

Fig. 1. Voluminous of the lipoma mass in the right inguinal region.
An ultrasound was performed at another hospital. In the ultrasound examination there was described a tumor which probably corresponds to the hernia in which a part of a omentum major and a part of bowel intestine is located. There was unable to view images from this examination.
The patient was taken to the operating room for a standard Lichtenstein hernia repair due to right inguinal hernia (fig. 2, 3). During surgical exploration of the inguinal area, there was no hernia but there was diagnosed a giant lipoma of the spermatic cord measuring 15 cm × 9 cm × 7 cm (fig. 4).
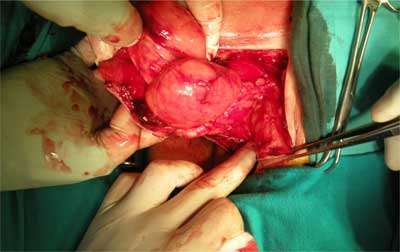
Fig. 2. Giant lipoma delivered from the inguinal region.
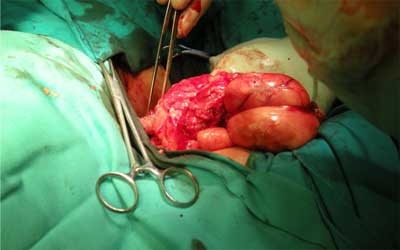
Fig. 3. Lipomatous mass.
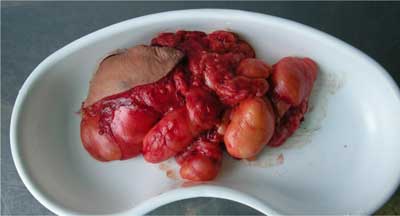
Fig. 4. The macroscopic appearance of an encapsulated fat tissue neoplasm.
Histopathology examination showed a well circumscribed piece of fatty tissue consistent with a benign lipoma. The postoperative period was uncomplicated and the patient left the ward in the second day after operation. At the 32-months follow-up, the patient has no evidence symptoms of recurrence lipoma.
DISCUSSION
Spermatic cord tumors are observed in 4% of all scrotal tumors (1, 3). The vast majority of these tumors (90%) are mesoderm origin (2, 3). Spermatic cord tumors are divided into these which located in the testicular tunica, epididymis or spermatic cord (4). 70% of neoplasms are benign and most of them are represented by lipomas (4). The etiology of is still unknown but lipomas of this region are the most common observed in the 4th and 5th decade of life (5). First time Tobin et al in 1946 described lipoma of the cord as a connective tissue between the peritoneum and the abdominal wall as consisting of three strata (6).
Lipomas of the spermatic cord are observed as a herniation of adipocytes (1-3). This fat herniation is the most frequent located from the retroperitoneal fat to the internal spermatic fascia (5). These tumors give the same symptoms as inguinal hernia and are detected when their growth reaches large size (5). Ultrasound, computer tomography and magnetic resonance imaging help identify lipomas before surgery (6).
During laparoscopic repair (TAPP – transabdominal preperitoneal) of inguinal hernia, lipomas of the spermatic cord may be unseen so it is advisable to perform gentle external compression to touch or see internal traction on the cord structures (7-9).
All lipomas of the spermatic cord must be removed because of the incidence of recurrence after inguinal hernia repair and due to a giant and long growth tumors can be converted into aggressive neoplasm – liposarcoma (7, 9).
CONCLUSIONS
1. Surgeon must examine the preperitoneal place and the structures of the cord for lipomas before the hernia operation;
2. In the case of obese patients or giant inguinal hernia, if there are doubts examining region of hernia, ultrasound of this region should be performed;
3. During a laparoscopic hernia repair exploration of the preperitoneal space is necessary because in other case surgeon can failed to recognize a lipoma of the spermatic cord, which can later mimicking a recurrent hernia;
4. Patients after surgical treatment of spermatic cord lipoma should be followed regularly.
Piśmiennictwo
1. Kaohsiung J: Giant lipoma of spermatic cord mimics irreducible inguinal hernia. Case report. Med Sc 2004; 20: 247-249. 2. Edelstein RA: Giant spermatic cord lipoma. The Scientific World Journal 2009; 9: 1194-1196. 3. Carrion Lopez P, Pastor Navarro H, Martinez Ruiz J et al.: Spermatic cord sarcomas: current status and report of four cases. Arch Esp Urol 2009; 62: 242-246. 4. Rodriguez Toves LA, Estebanez Zarranz J, Camacho Parejo J et al.: Paratesticular lipoma. Actas Urol Esp 1997; 21: 620-622. 5. Gersin KS, Heniford BT, Gracia-Ruiz A, Ponsky JL: Missed lipoma of the spermatic cord: a pitfall of transabdominal preperitoneal laparoscopic hernia repair. Surg Endosc 1999; 13: 585-587. 6. Tobin CE, Benjamin JA, Wells JC: Continuity of the fasciae lining the abdomen, pelvis and spermatic cord. Surg Gynecol Obst 1946; 83: 575-595. 7. Read RC, Schaefer RF: Lipoma of the spermatic cord, fatty herniation, liposarcoma. Hernia 2000; 4(3): 149-154. 8. Lan H, Loong F, Yuen WK, Patil NG: Management of herniated retroperitoneal adipose tissue during endoscopic extraperitoneal inguinal hernioplasty. Surg Endosc 2007; 21(9): 1612-1616. 9. Nasr AO, Tormey S, Walsh TN: Lipoma of the cord and round ligament: an overlooked diagnosis? Hernia 2005; 9: 245-247.
