© Borgis - New Medicine 2/2013, s. 47-49
*Konrad Wroński1, 2, Andrzej Lachowski2
Giant femoral lipoma causing venous obstructing syndrome – case report
1Department of Oncology, Faculty of Medicine, University of Warmia and Mazury in Olsztyn, Poland
Head of Department: prof. Sergiusz Nawrocki, MD, PhD
2Department of Surgical Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department: Andrzej Lachowski, MD
Summary
Lipoma is the most common benign neoplasm in the human body which develops from the adipose tissue. This tumors arise in subcutaneous tissues rather than deeper tissues where rare may cause compressive of some vein. The authors reported the case of femoral venous obstruction syndrome due to a giant femoral lipoma.
INTRODUCTION
Lipoma is the most common benign neoplasm in the human body which develops from the adipose tissue. It is estimated that about one percent of the general population has a lipoma. Lipomas are the most frequent found in middle age. Many lipomas are small with diameters of about 1-3 cm, but can enlarge to sizes greater than ten centimeters and are named “giant lipomas”. Giant lipomas located especially in the extremities can cause compression of the vein and cause chronic venous insufficiency.
The authors of this article report a rare case of giant lipoma which caused femoral venous obstruction syndrome due to compression. The authors found in PubMed Database several articles relating to that described problem (1-4).
CASE REPORT
The authors report the case of a 55-year-old woman who was referred to their department due to the presence of a large mass which was located on the right thigh. The tumor had been steadily increased in size from six months. The patient has reported pain, functional impairment and edema of the right leg for six months. There was no past history of deep vein thrombosis, surgery or trauma. On physical examination, the right limb had edema with early skin changes and in the medial-posterior part of the thigh was palpable giant tumor.
Doppler sonography was performed and integrated with MR. There was no old or new deep vein thrombosis or venous reflux and no lymphadenopathy. The mass of tumor caused compressing the femoral vein and venous obstruction. The MR scan showed a large sharply demarcated change of the focal length in the back of the thigh. The tumor lay between the great adductor muscle from the front and semitendinosus, semimembranosus and long head of the biceps thighs from behind. The tumor caused compression of the femoral vein and nerve (fig. 1). The cross sections of the tumor size was 10 x 5.5 cm, and 16 cm long axis (fig. 2).
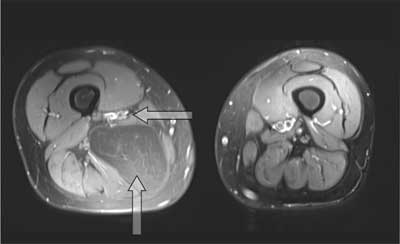
Fig. 1. The MR scan presents compression of the femoral vein and nerve caused by giant lipoma.
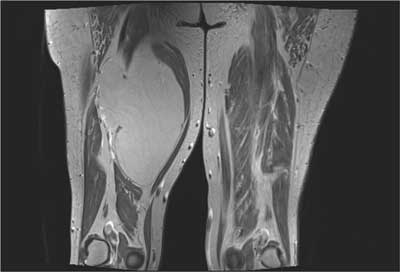
Fig. 2. The MR scan presents the size and localization of giant lipoma – the cross sections was 10 x 5.5 cm, and 16 cm long axis.
The patient was taken to the operating room for exploration and resection the tumor. The surgeons were prepared for a possible reconstruction of the artery, vein or femoral nerve. Upon opening the femoral sheath a well demarcated and encapsulated tumor was identified (fig. 3). The lipoma was dissected out and the vein and nerve were decompressed (fig. 4). After surgery there was no venous obstructing syndrome.

Fig. 3. The tumor lay between the great adductor muscle from the front and semitendinosus, semimembranosus and long head of the biceps thighs from behind.
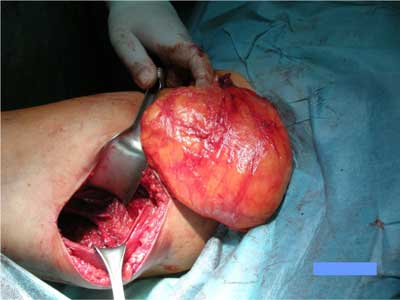
Fig. 4. The size of tumor after excision.
Histopathology examination showed a well circumscribed piece of fatty tissue consistent with a benign lipoma (fig. 5). The postoperative period was uncomplicated and the patient left the ward in the third day after operation.
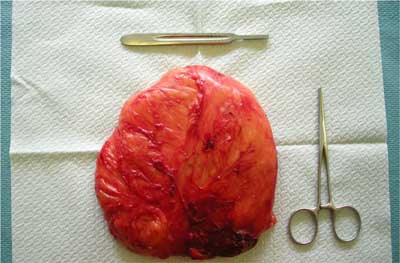
Fig. 5. Final histopathology showed a benign lipoma.
DISCUSSION
A giant lipoma (diameter greater than ten centimeters) occurring symptomatic venous syndrome is rare and the authors did not find such case in the medical literature. Chronic venous insufficiency (CVI) can be result of primary and secondary causes. The most common nonthrombotic causes of chronic venous insufficiency include external compression of ligaments, pelvic tumors, femoral hernia, retroperitoneal fibrosis, aneurysm and cysts (5). Giant lipoma causing femoral venous obstructing syndrome have not been previously reported. In this case giant lipoma caused significant compression effect to femoral vein flow and nerve resulting in leg swelling, pain and walking troubles. After surgery, the above described symptoms completely disappeared.
Every patient with a giant lipoma causing venous obstruction syndrome should be made Doppler sonography with imaging diagnostic – MRI or CT – allows to obtain accurate information on diagnosis and planning treatment.
The authors of this article believe that patients with giant lipomas of limbs that cause obstruction of large veins should be treated in the surgical wards with experience in similar operations, and vascular surgery. Lipomas can compress or invade the important vessels and in some cases it may be necessary to comply with the vessel reconstructive surgery. In the case of giant and long-standing lipomas may lead to transform into liposarcoma which was first time described by Wolgemuth in 1910. There have been a number of papers since that time describing such phenomenon, therefore patients with giant lipomas should be immediately directed at the surgical ward.
Piśmiennictwo
1. Day A, Thomas P: Femoral sheath lipoma causing venous obstruction syndrome. Ann R Coll Surg Engl 2010; 92(6): W21-22. 2. McClure MJ, Sarrazin J, Kapusta L et al.: Intravascular femoral vein lipoma: an unusual cause of lower limb venous obstruction. AJR Am J Roentgenol 2001; 176(2): 463-464. 3. Gasparis AP, Tsintzilonis S, Labropoulos N: Extraluminal lipoma with common femoral vein obstruction: a cause of chronic venous insufficiency. J Vasc Surg 2009; 49(2): 486-490. 4. Martin-Pedrosa JM, Del Blanco I, Carrera S et al.: Intravascular lipoma of the external iliac vein and common femoral vein. Eur J Vasc Endovasc Surg 2002; 23: 470-472. 5. Gasparis AP, Wall P, Ricotta JJ: Adventitial cystic disease of the external iliac vein presenting with deep venous thrombosis. A case report. Vasc Endovasc Surg 2004; 38: 273-276.
