© Borgis - Postępy Nauk Medycznych 7/2017, s. 351-356
*Arkadiusz Stasicki1, 2, Jan Bujok1, 3, Wojciech Biela1, 2, Anna Debudaj1, 4, Tomasz Ilczak1, 2, Michał Ćwiertnia1, 2, Beata Kudłacik1, Robert Kijanka1, 2, Piotr Białoń1, 5, Monika Chorąży6, Marzena Wojewódzka-Żelezniakowicz7, Robert Gałązkowski8, Kladiusz Nadolny9, 10, Jerzy Robert Ładny7, Rafał Bobiński1
Evaluation of medical rescue activities performed by Medical Rescue Teams in a patient with acute brain ischemia
Ocena medycznych czynności ratunkowych wykonanych przez zespoły ratownictwa medycznego u pacjenta w ostrym niedokrwieniu mózgu
1Institute of Emergency Medicine, Department of Nursing and Emergency Medicine, Faculty of Health Sciences, University of Bielsko-Biała
Head of Institute: Associate Professor Rafał Bobiński, MD, PhD
2Emergency Medical Services in Bielsko-Biała
Head of Services: Wojciech Waligóra
3Department of Neurosurgery, Independent Provincial Hospital in Bielsko-Biała
Head of Department: Janusz Krauze, MD, PhD
4Department of Anaesthesiology and Critical Care, Independent Provincial Hospital in Bielsko-Biała
Head of Department: Associate Professor Dariusz Maciejewski, MD, PhD
5Department of Emergency Medical Aid, Health Care Center in Żywiec
Head of Department: Antoni Juraszek
6Department of Neurology, Medical University of Białystok
Head of Department: Jan Kochanowicz, MD, PhD
7Department of Emergency Medicine and Disasters, Medical University of Białystok
Head of Department: Professor Jerzy Robert Ładny, MD, PhD
8Department of Emergency Medical Service, Medical University of Warsaw
Head of Department: Grzegorz Michalak, MD, PhD
9College of Strategic Planning in Dąbrowa Górnicza
Head of College: Anna Rej-Kietla, MD, PhD, LLM
10Institute of Public Health, Faculty of Public Health, Medical University of Silesia in Katowice
Head of Institute: Elżbieta Grochowska-Niedworok, PhD (Pharmacy)
Streszczenie
Wstęp. Na świecie każdego roku udar mózgu rozpoznawany jest u około 15 mln osób. Podstawą wdrożenia leczenia udaru niedokrwiennego mózgu jest przede wszystkim właściwe rozpoznanie, oparte na wykluczeniu innych zaburzeń o charakterze metabolicznym, które mogą manifestować podobne objawy kliniczne, oraz wykluczenie udaru krwotocznego. Pierwszy element łańcucha przeżycia, czyli wczesne rozpoznanie pacjenta w stanie zagrożenia życia i szybkie wezwanie służb ratowniczych, bez wątpienia ma wpływ na zminimalizowanie skutków udaru mózgu.
Cel pracy. Celem pracy jest ocena przeprowadzonych symulowanych działań Zespołów Ratownictwa Medycznego pod względem poprawności wykonania medycznych czynności ratunkowych u pacjenta z podejrzeniem udaru mózgu.
Materiał i metoda. Do badania włączono 42 zespoły ratownictwa medycznego, które brały udział w XII Międzynarodowych Mistrzostwach Polski w Ratownictwie Medycznym. Ocena wykonanych medycznych czynności ratunkowych była dokonywana w czasie rzeczywistym trwania zadania poprzez uzupełnianie przez sędziów mistrzostw przygotowanej karty oceny.
Wyniki. Oceniając układ krążenia, wszystkie 42 (100%) zespoły wykonały pomiar ciśnienia tętniczego krwi. 35 (83,3%) zespołów nie podało pacjentowi leków hipotensyjnych. 38 zespołów (90,5%) zakwalifikowało pacjenta do priorytetowego transportu do oddziału udarowego. 35 zespołów (83,3%) powiadomiło za pośrednictwem Dyspozytora Medycznego pracowników oddziału udarowego o transporcie pacjenta z podejrzeniem udaru niedokrwiennego mózgu.
Wnioski. Członkowie Zespołów Ratownictwa Medycznego prawidłowo wdrażają algorytm wytycznych postępowania z pacjentem z podejrzeniem udaru mózgu.
Summary
Introduction. Each year stroke is recognised in approximately 15 million people worldwide. Proper recognition based on exclusion of other metabolic disorders which may present similar clinical symptoms is primarily the basis for the implementation of treatment of ischemic brain stroke. The first element of the chain of survival, that is, early recognition of a patient with a life-threatening condition and fast call for emergency services with no doubt have influence on minimizing the consequences of brain stroke.
Aim. The aim of the study is the assessment of conducted simulated emergency activities of the Medical Rescue Teams in the scope of correctness of performing of medical rescue operations in a patient with suspected brain stroke.
Material and methods. 42 Medical Rescue Teams taking part in the XII International Polish Medical Rescue Championships were involved in the study. The assessment of the performed medical recue activities was made in real-time of duration of the task through the completing of the prepared evaluation card by the championships judges.
Results. Considering the cardiovascular system all 42 teams (100%) made a blood pressure measurement. 35 teams (83.3%) have not administered antihypertensive drugs to the patient. 38 teams (90.5%) qualified the patient for urgent transport to a stroke department. 35 teams (83.3%) notified the stroke department team about transporting a patient with suspected ischemic brain stroke via the Medical Dispatcher.
Conclusions. The members of the Medical Rescue Team properly implement the algorithm of guidelines of procedure with a patient with suspected brain stroke.

Introduction
The system of Emergency medical services was created to provide help to everyone who is in sudden threat to human health. The legislator precisely specifies the definition of sudden thread to human health as sudden or foreseeable occurrence of symptoms compromising the health status with possible serious injury of body functions or bodily injury, or, loss of human life as a direct consequence, requiring immediate medical rescue activities. The Act on the State Medical Rescue Services provides minimising the time that has elapsed from the occurrence of the sudden thread to human life to entering medical treatment at a specialist department (1).
Each year stroke is diagnosed at approximately 15 million people worldwide. From 4.6 to 5.7 million people die from brain stroke which constitutes 10% of overall deaths globally (2-4).
In developed countries brain stroke is the third leading cause of death, and the most common cause of the occurrence of disability in people aged over 40 (2, 5). Data collected by the World Health Organization (WHO) suggest that in 2015 brain stroke was the second cause of death of adults globally after the ischemic heart disease (6).
In Europe, Poland is second after the Russian Federation with the highest rate of deaths caused by strokes. The percentage level of deaths caused by strokes in Poland is two times higher than in Germany, France or Great Britain (7, 8).
Long-term consequences of brain stroke, that is, the necessity to provide the patient care of other people and rehabilitation cause generating the highest medical treatment costs of the commonly occurring disease entities. This is the reason why brain stroke causes a serious global economic problem (9).
In 2013 the American Heart Association and American Stroke Association updated the current definition of brain stroke. Brain stroke is defined as sudden occurrence of focal or generalised disorders of the brain function caused only by vascular causes related to the brain blood flow, lasting longer than 24 hours.
Stroke may also be recognized when:
– focal neurological symptoms last less than 24 hours, however, ischaemic focus was clearly documented using brain imaging techniques,
– the symptoms resolved after thrombolytic treatment, or the patient died within the first day from the onset of occurrence of the symptoms.
If the focal neurological symptoms resolve spontaneously before 24 hours pass and the ischemic focus is not observed any more in the brain imaging examination a transient ischemic brain attack is observed (TIA) (10, 11).
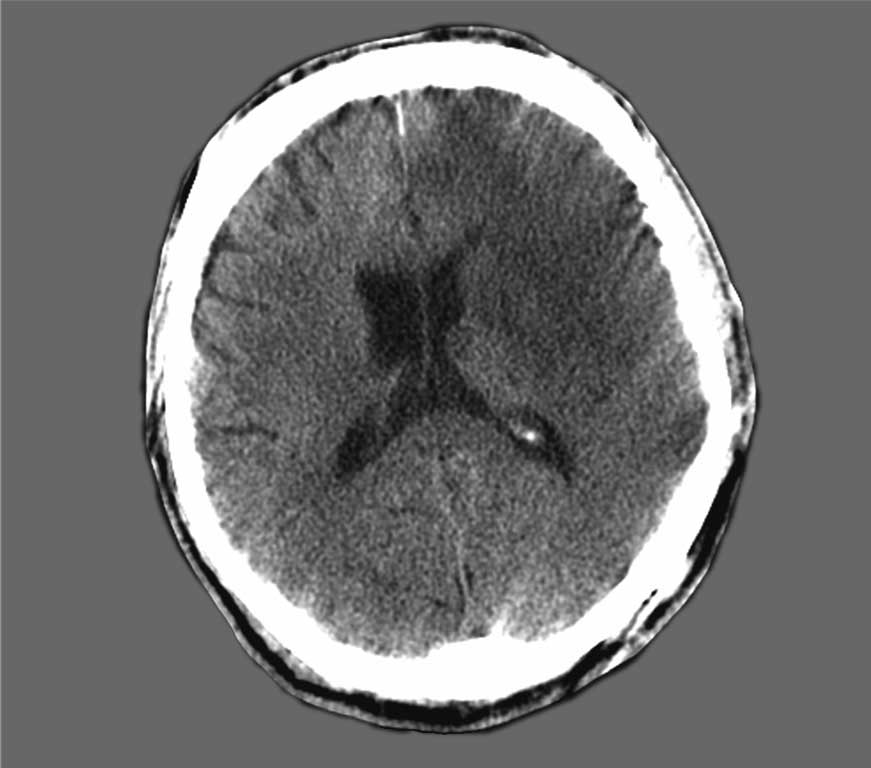
In the process of increasing of the stroke outbreak 2 millions of neurons are destroyed every minute (12). An example of results of computer tomography examination of a patient with ischemic brain stroke in the first and third day of hospitalization has been presented on figures 1 and 2. The pathogenic basis of a brain stroke are brain circulation disorders growing in time (in thromboembolic, embolic or hemodynamic mechanism) which cause gradual decline of perfusion in the brain and starting anaerobic glycolysis. The free radicals formed in this process cause damage of the blood-brain barrier and influx of plasma components to the extracellular compartment, which results in increasing of the volume of the brain, as a result of angiogenic and cytotoxic edema. The clinical symptoms of perfusion and biochemical disturbances and of the increase in brain volume, depending on the vascular eel affected by the attack are neurological loses (most often quantitative and qualitative disturbances of the state of consciousness, speech impairment, mobility deficits in the scope of cranial nerves and limbs). The basis for implementing treatment of ischemic brain stroke is firstly proper recognition based on excluding other metabolic disorders that may demonstrate similar clinical symptoms (e.g. hypoglycaemia, epileptic seizure, migraine) and exclusion of haemorrhagic stroke. A routine medical imaging conducted to this end is a computer tomography examination which ensures visibility of ischemic stroke characteristics: hypodense area covered with the stroke, blurring of the borders of the insula on the side of the stroke, increased electron density in the reach of the artery covered with the stroke and the head of the caudate nucleus on the side of the stroke, and the examination allows for excluding other pathology manifested by similar neurological symptoms (hematoma, brain tumour) (13).
Fig. 1. Computed-tomography of the head within the first 24 hours from the occurrence of the symptoms of the left middle cerebral artery ischemic stroke – hypodense area in the left frontal-temporal region. Patient aged 51 with clinical symptoms of aphasia, pyramidal paresis of right extremities and central paresis of nerve VII on the right
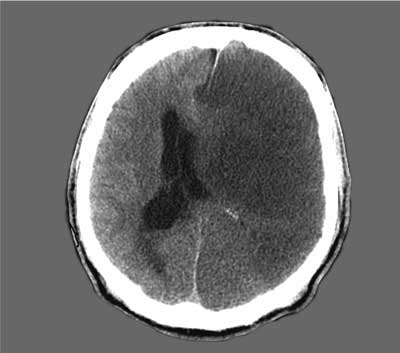
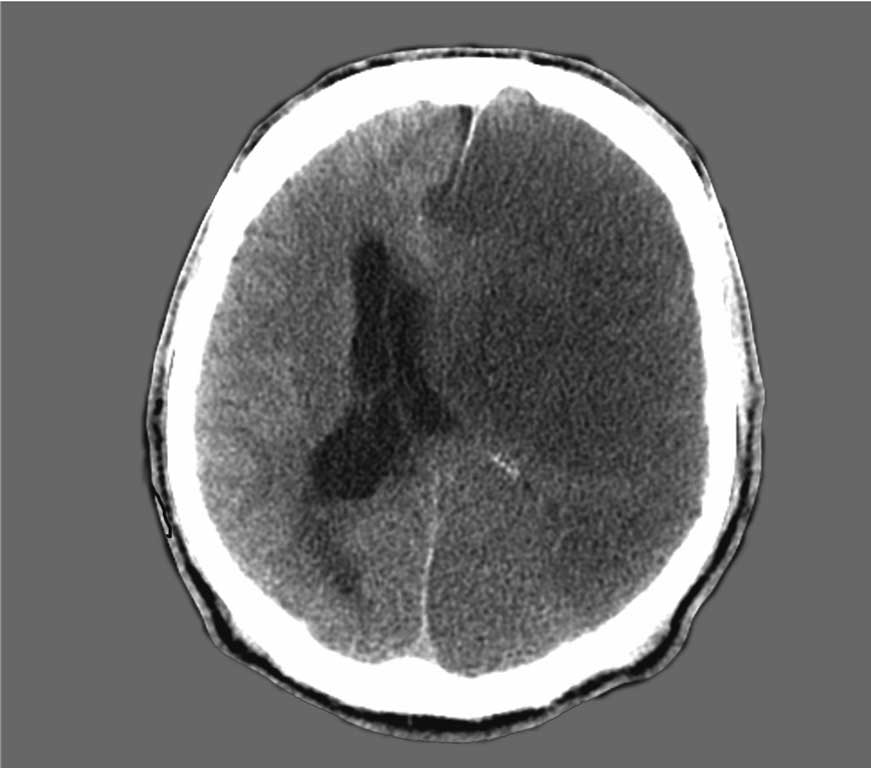
Fig. 2. Computed-tomography of the head within 72 hoursfrom the occurrence of the symptoms of the ischemic stroke in the patient from figure 1. Significant enlargement of the hypodense area within the scope of the left brain hemisphere with signs of brain edema (flattening of the gyri (ridges), narrowing of the sulci (grooves) at the convexity). Significant mass effect in the form of compression and displacement of the supratentorial ventricular system to the right
The key role in the treatment of ischemic stroke is played by the proceeding based on the possibility of recanalization of a closed vessel and reperfusion of areas covered with the ischemia as well as by the time that has elapsed from occurrence of the clinical symptoms till the moment of implementing the purposeful form of treatment.
Confirmation of the stroke is a basis for the application of intravenous thrombolysis with the use of the recombinant tissue plasminogen activator (rt-PA), if the time that has elapsed from occurrence of the symptoms of brain stroke shall not be longer than 4.5 hour, and, if the patient fulfils other criteria for application of this form of treatment (age 18-80, exclusion of haemorrhagic stroke, time of occurrence of symptoms at least 30 minutes and no substantial improvement after treatment). The form of the supply of rt-PA has influence on the possibility to prolong the time of recanalization of the closed vessel. In the event of intravascular interventions implemented by centres specialising in interventional neuroradiology the possibility of rt-PA supply directly to the artery affected by the thrombus through arteriography allows to prolong the time to 6 hours from the onset of occurrence of brain stroke symptoms. Results may be even more effective through mechanical thrombectomy (14-18).
In some cases when stroke symptoms are accompanied by large mass effect and the deteriorating neurological status of the patient the remaining solution is performing bone-meningeal decompression (19, 20).
The chain of survival used in emergency medicine (fig. 3) is a contractual definition of a few interdependent links that have influence on patients’ survival. The first element of the chain of survival, that is, early recognition of a patient with life thread and fast call for rescue services without any doubt have influence on minimising the effects of brain stroke (21). The subsequent links in the chain of survival in brain stroke are priority transport with previous notifying of the appropriate unit as well as fast making of the proper diagnosis and starting adequate treatment (3).
Fig. 3. “Chain of survival” in a patient with stroke (own elaboration)
The considerations for the functioning of the Emergency Medical Services should treat patients with symptoms that may indicate brain stroke with the highest priority.
A large proportion of patients and witnesses cannot recognize the symptoms that may indicate brain stroke which causes delay in entering specialised treatment (3).
Aim
The aim of the conducted simulated action of the Medical Rescue Teams was the assessment of the performed medical rescue activities in a patient with suspected brain stroke. The teams’ activities related to the classifying of a patient for immediate treatment at a specialised stroke department were assessed. The operations were assessed according to the Guidelines of the Group of Experts of the Vascular Diseases Section of the Polish Society of Neurology from the year 2012.
Material and methods
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Ustawa z dnia 8 września 2006 r. o Państwowym Ratownictwie Medycznym (Dz. U. 2016, poz. 1868).
2. Kaźmierski R: Diagnostyka i leczenie chorych w ostrej fazie udaru niedokrwiennego mózgu. Anest Ratow 2014; 8: 62-75.
3. Cichońska M, Morek M, Krawczyk W et al.: Ocena czasu od wystąpienia incydentu udaru mózgu do uzyskania pomocy medycznej w populacji regionu świętokrzyskiego. Pielęg XXI w. 2011; 3(36): 11-14.
4. Kaczorowski R, Murjas B, Bartosik-Psujek H: Rozwój i nowe perspektywy leczenia udaru w Polsce. Medical Review 2015; 13(4): 376-386.
5. Niewada M, Kamiński B, Kobaysahi A et al.: Koszty powtórnego udaru mózgu w Polsce. Farmakoter Psychiatr Neurol 2002; 2: 191-203.
6. The top 10 causes of death, dane WHO; http://www.who.int/mediacentre/factsheets/fs310/en/ (dostęp 7.04.2017).
7. Przygotowanie szpitali do leczenia pacjentów z udarem mózgu. Informacje o wynikach kontroli Najwyższej Izby Kontroli nr ew: 43/2016/P/15/072/LKA.
8. Ryglewicz D, Wiszniewska M, Cichy S et al.: Ischaemic strokes are more serve in Poland then in the United States. Neurology 2000; 54: 513-515.
9. Błaszczyk B, Czernecki R, Prędota-Panecka H: Profilaktyka pierwotna i wtórna udarów mózgu. Stud Med 2008; 9: 71-75.
10. Członkowska A: Nowa definicja udaru. Stanowisko American Heart Association i American Stroke Association 2013. Med Prakt 2014; 1: 42-46.
11. Sacco RL, Kasner SE, Broderick JP et al.: An updated definition of stroke for the 21 century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013; 44: 2064-2089.
12. Saver JL: Time is brain-quantified. Stroke 2006; 37: 263-266.
13. Kozubski W, Liberski P: Neurologia. PZWL, Warszawa 2006: 424-456.
14. Wiszniewska M, Kobayashi A, Członkowska A: Postępowanie w udarze mózgu. Skrót Wytycznych Grupy Ekspertów Sekcji Chorób Naczyniowych Polskiego Towarzystwa Neurologicznego z 2012 roku. Pol Przegl Neurol 2012; 8(4): 161-175.
15. Sang-Beom J, Younsuck K, Choi A, Kiwon L: Critical Care for Patients with Massive Ischemic Stroke. J Stroke 2014; 16(3): 146-160.
16. MA Y-D, Wang J, Du ZH et al.: Mechanical thrombectomy with solitaire stent for acute internal carotid artery occlusion without atherosclerotic stenosis: dissection or a cardiogenic thromboembolism. Eur Rev Med Pharmacol Sci 2014; 18: 1324-1332.
17. Li W, Yin Q, Xu G, Liu X: Treatment Strategies for Acute Ischemic Stroke Caused by Carotid Artery Occlusion. Interv Neurol 2016; 5: 148-156.
18. Kappelhof M, Marquering H, Berkhemer O et al.: Intra-arterial treatment of patients with acute ischemic stroke and internal artery occlusion: a literature review. J Neuro Intervent Surg 2015; 7: 8-15.
19. Vital BR, Hamamoto Filho PT, Luvizutto GJ et al.: Decompressive Hemicraniectomy in a South American Population-Morbidity and Outcomes Analysis. PLoS One 2016; 11(1): e0146747.
20. Baharvahdat H, Etemadrezaie H, Zabyhian S et al.: Decompressive craniectomy after unsuccessful intravenous thrombolysis of malignant cerebral infarction: Iran J Neurol 2014; 13(2): 101-104.
21. Monsieurs KG, Nolan JP, Bossaert L et al.: Podsumowanie Komitetu Wykonawczego ERC, Wytyczne Resuscytacji 2015. Polska Rada Resuscytacji, Kraków 2015: 5-13.
22. Kozera G, Raniszewska E, Gąsecki D, Nyka WM: Pierwsza pomoc u pacjentów z udarem mózgu. For Med Rodz 2007; 1(1):11-16.
23. Zalisz M: Postępowanie przedszpitalne z chorym na udar mózgu (w aspekcie leczenia trombolitycznego). Pol Ann Med 2009; 16(1): 160-167.
24. Zatońska K, Bolanowski M: Hipoglikemia jako problem diagnostyczny. Adv Clin Exp Med 2003; 12(3): 369-373.
25. Książkiewicz B, Gąsecki D: Leczenie we wczesnym okresie udaru mózgu. Chor Serca i Nacz 2006; 3(2): 83-90.