Michał Michalik, *Adrianna Podbielska-Kubera
Faciocranial complications of sinusitis
Powikłania twarzoczaszkowe zapalenia zatok
Department of Otolaryngology, MML Medical Centre, Warsaw, Poland
Head of Department: Michał Michalik, MD, PhD
Streszczenie
Zapalenie zatok to jedno z częściej występujących schorzeń. Jego etiologia nie jest do końca poznana, najczęściej dominują czynniki wirusowe i bakteryjne. Do głównych objawów należą: przekrwienie błony śluzowej nosa, obfita wydzielina z nosa, a także osłabienie węchu. Źródłem powikłań może być zapalenie w obrębie każdej zatoki. Powikłania rozwijają się najczęściej w wyniku zaostrzenia przewlekłego zapalenia zatok.
Zapalenie zatok może skutkować rozprzestrzenieniem się zapalenia do wnętrza czaszki lub w rejon oczodołów, zapaleniem kości i szpiku lub zakrzepicą zatoki strzałkowej górnej. Ze względu na anatomiczne położenie i bliskość istotnych struktur, zapalenie zatok klinowych może prowadzić do zapalenia opon mózgowych lub ropniaków podtwardówkowych, ropni płata skroniowego i zakrzepicy zatoki jamistej.
Grzybicze zapalenie zatok jest niezwykle niebezpieczne, bowiem charakteryzuje się szybko postępującym przebiegiem, często powikłanym rozsiewem wewnątrzczaszkowym i oczodołowym. Inwazyjne grzybicze zapalenie zatok przynosowych z powikłaniami oczodołowymi to stan zagrażający życiu. W przypadku obawy przed powikłaniem zapalenia zatok w obręb oczodołu lub wewnątrzczaszkowego oraz w przypadkach braku poprawy po zastosowaniu początkowej terapii empirycznej niezbędne jest wykonanie badań obrazowych, w tym tomografii komputerowej i rezonansu magnetycznego.
Wczesne diagnozowanie zapalenia zatok i multidyscyplinarne leczenie stanowiące połączenie antybiotykoterapii i leczenia operacyjnego, w tym neurochirurgii i zabiegów szczękowo-twarzowych, mogą skutecznie zapobiegać powikłaniom i znacznie zmniejszać zachorowalność i śmiertelność.
Summary
Sinusitis is one of the most common conditions. The aetiology of sinusitis has not been fully discovered; however, viruses and bacteria are usually the dominant causes. The chief symptoms include nasal congestion, profuse nasal discharge and a compromised sense of smell. Inflammation of any sinus can be the source of complications. Complications develop usually as a result of exacerbation of chronic sinusitis.
Sinusitis may result in inflammation spreading inside the cranium and to the orbital area and in the development of osteomyelitis or superior sagittal sinus thrombosis. Due to the anatomical location and proximity of important structures, sphenoid sinusitis may lead to meningitis or subdural empyemas, temporal lobe abscesses and cavernous sinus thrombosis.
Fungal sinusitis is very dangerous since it is characterised by a rapid course often complicated by intracranial and orbital spread. Invasive fungal paranasal sinusitis with orbital complications is a life-threatening emergency. If there is concern about possible orbital or intracranial complications of sinusitis or if there is no improvement after initial empirical therapy, the use of diagnostic imaging is necessary, including computed tomography and magnetic resonance imaging.
Early diagnosis of sinusitis and multidisciplinary management involving a combination of antibiotic therapy and surgical treatment, including neurosurgery and maxillofacial procedures can be effective in the prevention of complications and may significantly reduce morbidity and mortality.
Sinusitis
Sinuses are air cavities located in the facial cranium and near the nasal cavity and closely connected with it. Sinuses are lined with epithelium with cilia (1). Not all sinuses are present at birth. Ethmoid and maxillary sinuses are present and clinically significant already at birth. Sphenoid sinuses appear at three to seven years of age. Frontal sinuses are present only in 12% of newborns and develop at puberty (2).
Sinusitis is one of the most important and common diseases (3). It affects 20% of the population at different stages of life (4). Depending on the duration of the disease process sinusitis is divided into acute (lasting less than 12 weeks) and chronic (lasting over 12 weeks) (3). Sinusitis, particularly chronic sinusitis, significantly compromises the patient’s quality of life and generates high socioeconomic costs (5).
The aetiology of sinusitis is still being researched. The most common causes include nasal polyps, facial trauma, nasal septum deviation, respiratory infections, allergies and hay fever (6, 7). Periodontal disease may also be the source of inflammation (1).
Under physiological conditions, sinuses are sterile; however, they may be temporarily colonised by upper respiratory tract flora. Inflammation is most common in the maxillary sinuses. This is where odontogenic infections predominate as a result of close proximity of the teeth and sinuses (9). Bone structures constitute a barrier against the spread of infection to areas adjacent to the sinuses. However, complications develop in the event of bone damage, congenital or acquired bone abnormalities or haematogenous infection spread (2).
The majority of cases of sinusitis are secondary to upper respiratory and allergic infections. Bacterial sinusitis develops as a result of excessive bacterial growth in a closed sinus cavity. Inflammatory oedema creates an ideal environment for bacterial colonisation and growth since it hampers air exchange in narrow spaces. In addition, the activity of the mucociliary system becomes reduced, which compromises the natural protective barrier of the host and leads to discharge stasis (3).
The diagnosis of sinusitis is based on subjective symptoms, duration of symptoms and objective signs of inflammation (6). Nasal congestion, profuse nasal discharge and a compromised sense of smell are observed. The majority of sinusitis cases are viral infections, with no need for antibiotic therapy (7). However, the differentiation between a viral and bacterial infection is difficult: symptoms are similar and doctors prescribe antibiotic therapy. Sinusitis can also be caused by bacterial factors: Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Staphylococcus aureus, coagulase-negative staphylococci and Gram-negative bacteria: Pseudomonas aeruginosa, Proteus spp., Klebsiella spp., Enterobacter spp., Escherichia coli and anaerobic bacteria (Peptostreptococcus spp., Prevotella spp., Porphyromonas spp., Bacteroides spp.) (7). Anaerobic bacteria, which are characteristic for acute disease, are usually associated with dental infection. Fungi from the families Mucoraceae and Trichocomaenae (3) may be responsible for sinusitis in patients with a compromised immune system.
The head and neck contain a number of spaces which may become infected leading to life-threatening complications, including respiratory obstruction and neurological complications and to the spread of infection. Many of the early signs are subtle and may go unnoticed by the doctor (8). Local, orbital and intracranial complications may occur as a result of sinusitis (3).
Sinusitis complication risk factors
Bacterial infections of the central nervous system require quick diagnosis and immediate treatment. The most common bacterial infections observed at intensive care units include acute bacterial meningitis, subdural empyema, intracerebral abscess and encephalitis. Infections may be acquired outside of hospital or in hospital, for example after a neurosurgical procedure or they may be associated with cerebrospinal fluid drainage. Cerebral abscesses are often the result of chronic or metastatic infection foci such as otitis, sinusitis, pneumonia or endocarditis. The development of infection may result in serious systemic and neurological complications leading to high mortality or serious disability (9).
Sinusitis is common in patients at intensive care units and is usually secondary to nasotracheal or nasogastric intubation. Sinusitis in intubated patients may manifest exclusively as unexplained fever. Proptosis and orbital pain may suggest the presence of orbital complications (8).
Inflammation of any sinus can be the source of complications. Complications occur usually as a result of exacerbation of chronic sinusitis. However, they can also develop in acute viral and bacterial sinusitis, as a result of traumatic bone loss, endoscopic nasal and sinus surgery or incorrectly performed procedures using an external approach (3).
In the era of antibiotics purulent sinusitis is rare, but it does occur. Frontal sinusitis may result in inflammation spreading inside the cranium and to the orbital area, osteomyelitis or superior sagittal sinus thrombosis. Maxillary sinusitis may result in bone inflammation and destruction; intracranial spread is rare, except for nasal and cerebral mucormycosis. Due to the anatomical location and proximity of important structures, sphenoid sinusitis sometimes leads to meningitis or subdural empyemas, temporal lobe abscesses and cavernous sinus thrombosis (8).
Approximately 0.5-2% of viral upper respiratory infections are associated with secondary acute bacterial sinusitis and may rarely transform into more serious complications such as meningitis and intracranial abscess. The symptoms are often non-specific and include fever, headache, head skin tenderness, nausea and emotional disturbances (9).
The most common bacterial complications of acute sinusitis are orbital cellulitis and abscesses. Infections are most commonly caused by the bacteria S. pneumoniae, Streptococcus pyogenes and S. aureus and anaerobic bacteria; H. influenzae strains are less common (10). Widespread use of vaccines against H. influenzae and S. pneumoniae has lead to a decrease in the prevalence of sinusitis associated with these bacteria. However, infections associated with the presence of Streptococcus (e.g. S. anginosus) and Staphylococcus (e.g. S. aureus) are more commonly observed (11). Since infections of the oral cavity, head and neck, and abdomen with an initial S. anginosus aetiology are often multibacterial, it is assumed that orbital complications of sinusitis that includes S. anginosus may also be multibacterial (12).
A review of literature regarding the occurrence of sinusitis complications from the beginning of the previous century until now shows that intracranial complications of sinusitis are currently observed approximately four times less commonly than in previous years. However, the rate of certain complications, orbital for example, has not changed significantly. With the introduction of new-generation antibiotics, development of diagnostic techniques, improvement of surgical techniques and the use of neuronavigation, the rate of complications caused by intracranial infections has decreased. This change is also due to an increased awareness of patients of the need for sinusitis treatment. Permanent abnormalities such as epileptic seizures, paralysis, compromised mental abilities etc. are observed in approximately 30% of patients with intracranial complications of sinusitis (3).
Acute sinusitis is very common in the paediatric population. Secondary bacterial paranasal sinusitis occurs in 6-9% of all cases of viral upper respiratory infections in children. The majority of infections are uncomplicated and some of them can be treated without antibiotics. Sometimes acute sinusitis may be associated with serious orbital and intracranial complications (13). It is estimated that in 5% of paediatric patients with acute sinusitis infection may spread beyond the sinuses directly or via the bloodstream (12).
Ethmoid sinusitis may lead to orbital complications, which are more common in younger children since ethmoid sinuses are already developed at birth. Intracranial complications are more commonly observed in older children and are secondary to frontal sinusitis (2). Children with acute bacterial sinusitis complications have an increased risk of morbidity and mortality. In addition, children from families with a lower socioeconomic status do not always enjoy a full access to primary healthcare, including vaccinations; they are also diagnosed at later stages of disease, which is associated with longer hospital stay and increased mortality (2).
Complications of paranasal sinusitis involving the orbits and the inside of the cranium occur relatively rarely, but are a serious threat to the health and life of the patient (14). The prevalence of intracranial complications is 3 to 10% (3). Clayman et al. (15) recorded a 3.7% prevalence of intracranial complications of paranasal sinusitis in children. A more recent study suggests that the prevalence of orbital and intracranial complications of sinusitis may be as high as the sinusitis patient hospitalisation rate (3-5%) (13). The proximity of the orbits and the brain makes it possible for the infection to spread in a direct manner. Quick diagnosis of the initial stages of complications and starting appropriate treatment in a short period of time remain the most important issues. This is particularly difficult in intracranial complications, since their symptoms may be non-specific at the early stages, but they do develop rapidly and may lead to serious consequences, including strong extraocular pain, high fever, meningitis, ophthalmoplegia and blindness (14). The spread of sinusitis into the orbital area usually occurs according to the pattern described by Chandler et al. in 1970 and involves the following conditions one by one: preseptal cellulitis, orbital cellulitis, subperiosteal abscess, orbital abscess and cavernous sinus thrombosis. Orbital complications represent a risk of vision loss (12).
If such symptoms as headaches, fever, neurological manifestations, seizure activity and impaired consciousness with a rapid progress occur, various possible causes should be considered and differential diagnosis should be made between viral meningitis and encephalitis, different forms of bacterial meningitis, cerebral vessel thrombosis, encephalitis and abscesses of non-cerebral origin, e.g. otogenic abscesses. Sinusitis-related bacterial meningitis is usually associated with loss of consciousness, epileptic seizures and increased intraocular pressure. If no fever is observed, differential diagnosis should mainly include primary and metastatic brain tumours, stroke and subdural haematomas (3).
In the area where the bone wall tightly adheres to the dura, extradural abscesses are observed between the internal surface of the posterior bone wall of the frontal sinus and the dura. Infection may be transferred to the dura with the development of an epidural and/or subdural empyema (3).
Subdural empyemas are characterised by a severe clinical course, which may be due to the fact that the subdural space does not contain any barriers which could stop the spread of infection. Streptococci, staphylococci and anaerobic bacteria are the most common pathogens associated with intracranial complications of sinusitis (3). Subdural empyemas are observed much more often in young men. This may be due to anatomical differences in paranasal sinuses and the frontal bone. A subdural empyema is a collection of pus which occurs usually as a result of sinusitis; it may also spread from an extradural empyema. The subdural space is large and includes few barriers that could stop the spread of infection. Cooperation between doctors from different fields, e.g. a neurologist and a neurosurgeon is very important since some complications produce non-specific symptoms. Nuchal rigidity may be an atypical sign of a peripheral empyema and brain abscesses suggesting the possible development of a subdural empyema (3).
Brain abscesses are focal infections in the brain tissue. In patients with normal immunity, a tight blood-brain barrier and good vascularisation of meninges make the brain tissue relatively highly resistant to infection. However, in bacterial invasion, brain tissue inflammation (encephalitis) develops at the first stage and, at the last stage, a closed abscess forms. Patients complain of various symptoms which evolve as the disease progresses; the symptoms usually last from a few days to a few weeks and include headache, fever, neurological manifestations, epileptic seizures, personality changes, orientation disorders, dementia and drowsiness. In the case of brain abscesses located deeper in the frontal and parietal lobes, hemiparesis on the contralateral side is observed (3).
Allergic fungal sinusitis (AFS) is a type of sinus colonisation by various saprophytic fungi. It is a chronic form of sinusitis commonly observed in young atopic patients with normal immunity. The majority of patients have polyps in the nasal cavity. The patients develop an allergic reaction to mycelial fragments and produce a thick mucus. Allergic fungal sinusitis may lead to bone erosion or expansion of the allergic fungal mass to the orbital area and subsequently to the brain (16).
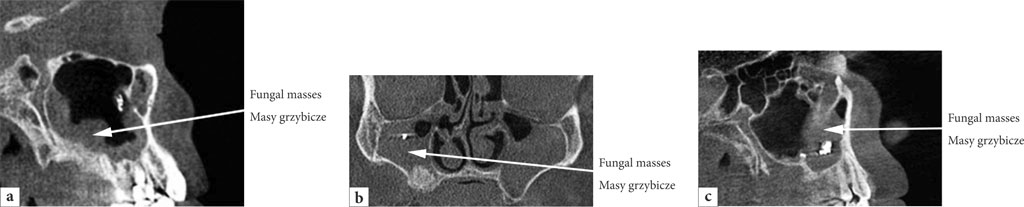
Fungal sinusitis is characterised by a rapid course often complicated by intracranial and orbital spread. It is most common in patients with compromised immunity and those with diabetes (8). Diabetes is the most frequent primary risk factor for invasive fungal paranasal sinusitis with orbital complications (80%) (17). Invasive fungal paranasal sinusitis with orbital complications is a life-threatening emergency, with a mortality rate as high as 80%. Diagnostic investigation using standard rhinoscopy may not reveal certain anatomical structures. It is computed tomography of the sinuses that is the right tool for the diagnosis of invasive fungal sinusitis with orbital complications (17). Opaque soft tissue, thickened mucosa and bone damage are observed on a computed tomography scan (8). Examples of developing fungal masses following dental and periodontal treatment are shown in figures 1a-c (the authors’ own materials).

Fig. 1a-c. Development of fungal masses following dental and periodontal treatment
The most serious complication of AFS is vision loss. It is assumed that the mechanism of vision loss is secondary to direct optic neuritis (16). The main symptoms include headache, fever and facial oedema. In the case of intracranial complications, seizures, decreased level of consciousness and coma also occur (8). According to Alaraj et al. (16), orbital symptoms occur in approximately 17% of patients with AFS. The most common signs and symptoms include proptosis, double vision, ptosis, vision loss and ophthalmoplegia. The treatment of choice in such cases includes surgery, oral steroid therapy and subsequently nasal steroids.
Diagnosis and treatment of sinusitis complications
Diagnostic imaging is required if there is a concern about possible orbital or intracranial complications of sinusitis and if initial empirical therapy brings no improvement (8).
Computed tomography (CT) and magnetic resonance imaging (MRI) are currently the most reliable and least invasive methods for the diagnosis and monitoring of intracranial infections (3). Plain sinus films may reveal signs of acute sinusitis, but CT provides better visualisation of sinuses, particularly ethmoid and sphenoid sinuses. A contrast-enhanced CT scan is the best method of visualising orbital complications. MRI is extremely useful in the examination of intracranial complications (8). Magnetic resonance imaging is better than computed tomography in the visualisation of abscesses at early stages of development. MRI scans of the brain make it possible to determine the location and shape of the abscess, the presence of oedema in the surrounding brain tissue and the presence of associated subdural empyemas, and to monitor treatment efficacy (3).
Orbital complications categorised by Chandler require early diagnosis and aggressive treatment. The severity of complications and their cause are determined using rhinoendoscopy, ophthalmic examination and sinus CT (18).
It is not possible to determine a relationship between sinusitis and periodontal disease using routine dental examination. Cone beam computed tomography (CBCT) is a much more sensitive technique in the detection of a relationship between periapical dental lesions and lesions present in the sinuses (4).
Even though the methods used for the treatment of acute and chronic sinusitis are often various, the methods used for the treatment of intracranial complications must be clear, unambiguous and performed immediately. The aim of the treatment is to eliminate the focus of inflammation in the sinuses and remove intracranial inflammatory lesions.
Typical treatment of intracranial complications of sinusitis includes endoscopic removal of inflammatory lesions in the nose and the sinuses with concomitant removal of a purulent intracranial leak. Frontal lobe abscesses and subdural abscesses are mainly treated using a closed method involving drainage. Treatment efficacy can be increased by the use of neuronavigation. In the cases where an abscess is located in close proximity to the dura, surgery needs to be performed in cooperation with a neurosurgeon. All procedures are conducted after the initiation of wide-spectrum antibiotic therapy (3).
The majority of clinicians treat early orbital complications and cellulitis with oral antibiotics (14). Laboratory and ophthalmic monitoring is mandatory. Oedema, ocular pain, profuse discharge and a lack of improvement after the administration of oral antibiotics are indications for intravenous antibiotic therapy or a surgical procedure (18). Historically, the presence of a subperiosteal or orbital abscess was an indication for surgical drainage apart from antibiotic therapy. Research has shown that empirical antibiotic therapy (ampicillin-sulbactam) administered for 24-48 hours and subsequent targeted therapy are effective in many cases. In communities with a high prevalence of methicillin-resistant Staphylococcus aureus (MRSA) the type of antibiotic therapy used may be modified accordingly (14).
Surgical intervention is indispensable in the event of visual acuity reduction, abscesses, deterioration of the patient’s clinical status and a lack of improvement after 48 hours of antibiotic treatment. In the case of a subperiosteal orbital abscess, the use of wide-spectrum intravenous antibiotics (clindamycin and ceftriaxone) should be started together with an ophthalmologist consultation (14). If the results of eye examination indicate the presence of mild lesions, intravenous antibiotic therapy should be continued in parallel with daily ophthalmic follow-up. If the patient’s clinical status does not improve or ophthalmic examination shows deterioration, surgical drainage should be performed, which is usually possible to conduct endoscopically. The orbital periosteum is usually not interfered with. In rare cases in which endoscopic drainage is not possible, ethmoidectomy with external drainage is performed (14).
The use of anticoagulation therapy in cavernous sinus thrombosis is a matter of controversy. It seems, however, that the administration of heparin at suitable doses, removal of inflammatory lesions in the sinuses, wide-spectrum antibiotic therapy and appropriate hydration allow the patient to recover sooner (3).
The treatment of acute fungal sinusitis is usually a combination of surgical methods and postoperative oral and nasal steroid administration. In the majority of cases this treatment regimen works well (16). Invasive fungal infections with orbital and intracranial involvement usually require surgical intervention (8).
Case reports
The prevalence of intracranial complications of sinusitis varies across the clinical material. Before the use of antibiotics the most common complications included meningitis and subdural empyema associated with ethmoid and frontal sinusitis.
In a study by Clayman et al. (15), intracranial complications accounted for 3.7% of cases among 649 patients admitted to hospital due to sinusitis. In 2000-2013 Szyfter et al. observed frontal lobe abscesses in 9 patients with sinusitis-related complications. This figure accounted for 43% of cases of sinusitis in that time period. In addition, epidural abscesses were confirmed in 24% of cases and subdural abscesses were confirmed in 19% of cases. Frontal lobe abscesses were diagnosed in 50% of patients with intracranial complications of sinusitis. These patients represented the largest group of patients with intracranial complications of sinusitis (3).
Sedaghat et al. (19) conducted statistical analysis of sinusitis complications. A complication was confirmed in less than 1% of patients with acute bacterial sinusitis. The majority of patients hospitalised for an emergency condition had orbital complications (76%); preseptal cellulitis was observed in 15% and intracranial complications were observed in 9% of patients. Dugar et al. (20) made a hypothesis that a lower economic status and inadequate access to preventive measures led to prolonged hospitalisation and increased mortality in patients with sinusitis complications.
Schupper et al. (13) analysed 16 paediatric cases of intracranial complications of acute sinusitis. The majority of the patients were teenagers; the symptoms were related to frontal and ethmoid sinuses and included headaches and fever. No cranial defects, including trauma to the base of the skull, neoplasms, previous surgical procedures and congenital defects were found in any of the patients. Successful treatment was conducted using endoscopic sinus surgery in combination with a neurosurgical procedure. Among individuals with reinfection, anaerobic bacteria were cultured as the dominant species in 66.7% of cases. This suggests that anaerobic organisms may not be sufficiently covered in the currently used antibiotic regimens or they display increased virulence. In addition, the presence of anaerobic infections in intracranial cultures was associated with an increased number of craniotomies and prolonged antibiotic therapy (13).
Ginat et al. (21) presented a case of a patient with a history of hypertension who developed left-sided headache. He was initially treated with sumatriptan. The headaches gradually worsened. Contrast-enhanced computed tomography revealed extensive opacification of the left maxillary sinus, a fluid collection and extensive oedema and erosion of the posterior wall of the left maxillary sinus. The patient developed jaw spasm, fever of up to 39.3°C, left-sided oedema, upper lip numbness, tachycardia and leukocytosis. The patient did not confirm any facial trauma or dental procedures in the past. The results of microbiological testing confirmed the presence of Gram-positive cocci and bacilli. Acute bacterial sinusitis with bone erosion and a medial abscess of the masticatory system without a confirmed odontogenic disease were diagnosed. Drainage was performed and subsequently the sinus was surgically cleaned and antibiotic therapy was administered (21).
Šuchaň et al. (18) evaluated 8 patients with suspected orbital complications who were admitted to hospital in 2008-2013. The causes of orbital complications was acute and chronic sinusitis, particularly ethmoid sinusitis (62.5%); maxillary (25%) and frontal sinusitis (12.5%) were also diagnosed. Multiple sinus involvement was most commonly diagnosed (75%). In 37.5% of cases, periorbital oedema/preseptal orbital cellulitis and in 25% of cases a subperiosteal abscess was diagnosed. In half of the cases, the dominant pathogens were S. epidermidis and S. aureus. The patients had mainly the following symptoms: periorbital oedema (100%), proptosis, chemosis (50%), double vision and glaucoma (12.5%). Combination treatment including antibiotic therapy and surgical treatment was used in all patients. Quick improvement was achieved and mean hospitalisation time was 7 days (18). Individuals who see a specialist a few weeks after the onset of vision deterioration are at risk of permanent vision loss. Carter et al. (22) reported a case of temporary vision loss; the patient regained their vision after surgery. Gupta et al. (23) presented 4 cases of vision loss; 3 patients completely regained their sight and one regained their sight partially (16). The cases reported show how important early diagnosis and aggressive combination therapy are. Such action may prevent vision loss and life-threatening complications (18).
Altman et al. (24) noted that young men with frontal paranasal sinusitis are at an increased risk of rapidly developing intracranial complications and should receive more aggressive treatment. A review of data from an American hospital shows that approximately a half of patients admitted due to sinusitis-related intracranial abscesses were children aged 10 to 15 years. In a large study involving adults as well, Clayman et al. (15) demonstrated that intracerebral abscesses located in the frontal lobe were diagnosed most frequently (3).
Over 12 years of research Rosenfeld and Rowley (25) discovered 9 cases of intracranial complications of sinusitis in children aged 2 to 16 years. The peak incidence was at the age of approximately 14 years with a predominance of boys (7 out of 9). The most common symptoms included: fever (67%), headaches (67%) and rhinitis (22%).
Miloundja et al. (26) conducted a review regarding children treated for cranioencephalic complications of sinusitis. In the analysed period 58 children with sinusitis were hospitalised; in 8 of them (13.8%) cranioencephalic complications were confirmed. The mean age of the children was 13 years. The symptoms developed for 14 days on average (3-45 days). The main symptoms included febrile headaches and neurological manifestations; the sinuses were tender. Impaired consciousness was confirmed in five cases. In 5 children a subdural empyema developed; in addition, thrombophlebitis of the sagittal sinus, brain abscess with thrombophlebitis of the sagittal sinus and meningitis with thrombophlebitis of the sagittal sinus were confirmed. Two children had osteomyelitis at the frontal sinus, including a frontal lobe abscess; in one child multiple brain abscesses were diagnosed. In five children concomitant sinus and neurosurgical drainage was performed; in two children only sinus drainage was conducted and in one child neurosurgical drainage was exclusively performed. Microbiological culture tests were positive for Streptococcus equinus (one case), S. aureus (one case), S. pneumoniae and H. influenzae (one case), and Aerococcus viridans (one case). In 4 cases the treatment was successful, in 3 cases recurrence was observed and one patient died. Coudert et al. (27) confirmed the presence of Streptococcus species in 60% of orbital abscesses and Miah et al. (28) reported the presence of S. anginosus in 61.3% of patients with orbital and intracranial complications. A study by Peña et al. (29) indicates the predominance of Staphylococcus species (47%). In a study by Miah et al. (28), S. anginosus was the dominant species. Another pathogen was S. aureus. Other researchers, including Hamill et al. (30) also report the predominance of S.aureus among paediatric patients with acute sinusitis-related complications. McKinley et al. (31) confirmed that S. aureus was the most commonly isolated pathogen in patients with orbital complications of acute sinusitis; the majority of S.aureus strains were methicillin-resistant (72.3%).
In patients with severe symptoms and complications of acute sinusitis wide-spectrum antibacterial agents are recommended which act against Streptococcus strains, Staphylococcus species (including MRSA) an anaerobic bacteria (11). Over 60 years ago sinusitis was commonly treated with penicillin and/or sulphonamides and H. influenzae strains dominated in the majority of intracranial infections. The use of wider-spectrum antibiotics has lead to a decrease in the number of intracranial complications of acute paranasal sinusitis in children and adolescents. The types of microbes responsible for these infections have also changed. Staphylococci and streptococci have started to predominate. Schupper et al. (13) noted that the presence of a few bacterial species in sinusitis is associated with an increased number of days spent in hospital, higher rates of abscess recurrence and longer duration of antibiotic use. Multibacterial cultures may be predictive in identifying higher-risk patients who will require more intensive treatment regimens for infections. The introduction of vaccines against type B H. influenzae and S. pneumoniae has reduced the number of cases of complications caused by these bacteria to practically zero (11). The association between the presence of Streptococcus and a longer hospital stay and the need for neurosurgical intervention noticed by the authors may support the idea that infections caused by these bacteria are difficult to treat (11).
Based on data from South Africa, Mortimore et al. (32) indicate that the most common microorganism culture obtained in orbital or intracranial complications of sinusitis was S.anginosus. These results are corroborated by Rudloe et al. (33). Viridans group streptococci (VGS), including S.anginosus, may have a synergistic relationship with oral anaerobic bacteria, which increases their virulence. This is observed in sinusitis complications, among other conditions. A question remains whether inadequate oral hygiene is a risk factor for acute sinusitis complications through the promotion of S.anginosus growth in synergy with anaerobic bacteria (12).
The presence of fungal cells in the nasal cavity may lead to septal mucosa compression and a compromised blood flow to the septal epithelium. This, in turn, may cause septal necrosis and perforation (34). Lee et al. (34) presented a case of a 75-year-old man with chronic nasal obstruction and purulent nasal discharge. A 2-month treatment administered before did not bring any improvement. Endoscopic nasal examination revealed a large polypous mass and a large amount of pus in the right nasal cavity. After partial pus removal using suction, a dark-brown material was found on the right side. Computed tomography confirmed the presence of soft tissue. Based on suspicion of fungal sinusitis, endoscopic sinus surgery was performed. The presence of mycelium was confirmed using tests. Nasal septum perforation was observed in the patient, which is a rare complication of invasive fungal sinusitis.
Conclusions
Early diagnosis of sinusitis and multidisciplinary management involving a combination of antibiotic therapy and surgical treatment, including neurosurgery and maxillofacial procedures can be effective in the prevention of complications and may significantly reduce morbidity and mortality.
Orbital and intracranial complications are characterised by a good long-term prognosis which becomes worse with a prolonged hospital stay. Early diagnosis and adequate medical intervention may reduce the need for intravenous antibiotic therapy and aggressive forms of treatment.
Quick neurological assessment and imaging studies should be performed if intracranial abscesses are suspected. The most effective diagnostic method in such cases is magnetic resonance imaging.
Invasive fungal paranasal sinusitis with orbital complications is characterised by high mortality. Treatment success depends on the patient’s awareness of risk factors and on sufficiently early identification of the symptoms. The diagnosis of invasive fungal paranasal sinusitis with orbital complications is usually delayed due to the long time necessary to identify the fungi. Early identification of fungal factors will make it possible to provide earlier and more precise treatment, giving patients a better prognosis. An aggressive surgical procedure is usually indispensable. It is very important to identify the relationship between proptosis and sinusitis in patients with fungal sinusitis. Ophthalmologists with a broad knowledge and experience play a key role in this.
Even though extradural abscesses secondary to sinusitis are relatively rare, the knowledge of these potentially life-threatening complications should be increased in order to ensure optimal and timely treatment. In addition, the treatment of complications generates significant costs for the healthcare system. It involves the use of advanced imaging techniques, longer hospital stays and surgical procedures. Appropriate understanding of the microbiology of sinusitis is important.
The high pathogenic potential of S. anginosus strains and their combination with oral anaerobic bacteria beg the question whether adequate oral hygiene may prevent orbital complications of sinusitis. There is evidence to confirm that mechanical cleaning procedures and antibacterial mouthwash liquids reduce the microbial count in the oral cavity.
Piśmiennictwo
1. Onişor-Gligor F, Lung T, Pintea B et al.: Maxillary odontogenic sinusitis, complicated with cerebral abscess – case report. Chirurgia (Bucur) 2012; 107(2): 256-259.
2. Mehta VJ, Ling JD, Mawn LA: Socioeconomic Disparities in the Presentation of Acute Bacterial Sinusitis Complications in the Pediatric Population. Semin Ophthalmol 2016; 31(4): 405-408.
3. Szyfter W, Kruk-Zagajewska A, Bartochowska A, Boruck Ł: Intracranial complications from sinusitis. Otolaryngologia Polska 2015; 69(3): 6-14.
4. de Lima CO, Devito KL, Baraky Vasconcelos LR et al.: Correlation between Endodontic Infection and Periodontal Disease and Their Association with Chronic Sinusitis: A Clinical-Tomographic Study. J Endod 2017; 43(12): 1978-1983.
5. Halawi AM, Smith SS, Chandra RK: Chronic rhinosinusitis: epidemiology and cost. Allergy Asthma Proc 2013; 34(4): 328-334.
6. Manes RP, Batra PS: Etiology, diagnosis and management of chronic rhinosinusitis. Expert Rev Anti Infect Ther 2013; 11(1): 25-35.
7. Stevens WW, Lee RJ, Schleimer RP, Cohen NA: Chronic rhinosinusitis pathogenesis. J Allergy Clin Immunol 2015; 136(6): 1442-1453.
8. Jaworsky D, Reynolds S, Chow AW: Extracranial head and neck infections. Crit Care Clin 2013; 29(3): 443-463.
9. Henriksen P, Yazdanyar N, Schmidt LS, Frederiksen MS: Epidural abscess secondary to sinusitis. Ugeskr Laeger 2016; 178(52): pii: V10160754.
10. Haas H, Lorrot M, Hentgen V et al.: Antibiotherapy of severe ENT infections in children: complicated sinusitis. Arch Pediatr 2013; 20 (suppl. 3): e5-9.
11. Mulvey CL, Kiell EP, Rizzi MD, Buzi A: The Microbiology of Complicated Acute Sinusitis among Pediatric Patients: A Case Series. Otolaryngol Head Neck Surg 2019; 160(4): 712-719.
12. Flam JO, Platt MP, Sobel R et al.: Association of oral flora with orbital complications of acute sinusitis. Am J Rhinol Allergy 2016; 30(4): 257-260.
13. Schupper AJ, Jiang W, Coulter MJ et al.: Intracranial complications of pediatric sinusitis: Identifying risk factors associated with prolonged clinical course. Int J Pediatr Otorhinolaryngol 2018; 112: 10-15.
14. Nocon CC, Baroody FM: Acute Rhinosinusitis in Children. Curr Allergy Asthma Rep 2014; 14(6): 443.
15. Clayman GL, Adams GL, Paugh DR, Koopmann CF Jr: Intracranial complications of paranasal sinusitis: a combined institutional review. Laryngoscope 1991; 101: 234.
16. Alaraj AM, Al-Faky YH, Alsuhaibani AH: Ophthalmic Manifestations of Allergic Fungal Sinusitis. Ophthalmic Plast Reconstr Surg 2018; 34(5): 463-466.
17. Piromchai P, Thanaviratananich S: Invasive Fungal Rhinosinusitis versus Bacterial Rhinosinusitis with Orbital Complications: A Case-Control Study. Scientific World Journal 2013; 2013: 453297.
18. Šuchaň M, Horňák M, Kaliarik L et al.: Orbital complications of sinusitis. Cesk Slov Oftalmol 2014; 70(6): 234-238.
19. Sedaghat AR, Wilke CO, Cunningham MJ, Ishman SL: Socioeconomic disparities in the presentation of acute bacterial sinusitis complications in children. Laryngoscope 2014; 124: 1700-1706.
20. Dugar DR, Lander L, Mahalingam-Dhingra A, Shah RK: Pediatric acute sinusitis: Predictors of increased resource utilization. Laryngoscope 2010; 120: 2313-2321.
21. Ginat DT, Lee SK, Baroody F: Headaches of otolaryngological origin. Eur Ann Otorhinolaryngol Head Neck Dis 2016; 133(3): 209-210.
22. Carter KD, Graham SM, Carpenter KM: Ophthalmic manifestations of allergic fungal sinusitis. Am J Ophthalmol 1999; 127: 189-195.
23. Gupta AK, Bansal S, Gupta A et al.: Visual loss in the setting of allergic fungal sinusitis: pathophysiology and outcome. J Laryngol Otol 2007; 121: 1055-1059.
24. Altman KW, Austin MB, Tom LW et al.: Complications of frontal sinusitis in adolescents: case presentations and treatment options. Int J Pediatr Otorhinolaryngol 1997; 41: 9-20.
25. Rosenfeld EA, Rowley AH: Infectious intracranial complications of sinusitis, other than meningitis, in children: 12-year review. Clin Infect Dis 1994; 18(5): 750-754.
26. Miloundja J, Bamba JS, Mouba JF et al.: Cranioencephalic complications of bacterial sinusitis in children and adolescents: eight cases in Libreville (Gabon). Sante 2011; 21(4): 215-220.
27. Coudert A, Ayari-Khalfallah S, Suy P, Truy E: Microbiology and antibiotic therapy of subperiosteal orbital abscess in children with acute ethmoiditis. Int J Pediatr Otorhinolaryngol 2018; 106: 91-95.
28. Miah MS, Nix P, Koukkoullis A, Sandoe J: Microbial causes of complicated acute bacterial rhinosinusitis and implications for empirical antimicrobial therapy. J Laryngol Otol 2016; 130: 169-175.
29. Peña MT, Preciado D, Orestes M, Choi S: Orbital complications of acute sinusitis: changes in the post-pneumococcal vaccine era. JAMA Otolaryngol Head Neck Surg 2013; 139: 223-227.
30. Hamill CS, Sykes KJ, Harrison CJ, Weatherly RA: Infection rates of MRSA in complicated pediatric rhinosinusitis: an up to date review. Int J Pediatr Otorhinolaryngol 2018; 104: 79-83.
31. McKinley SH, Yen MT, Miller AM, Yen KG: Microbiology of pediatric orbital cellulitis. Am J Ophthalmol 2007; 144: 497-501.
32. Mortimore S, Wormald PJ, Oliver S: Antibiotic choice in acute and complicated sinusitis. J Laryngol Otol 1998; 112: 264-268.
33. Rudloe TF, Harper MB, Prabhu SP et al.: Acute periorbital infections: Who needs emergent imaging? Pediatrics 2010; 125: e719-e726.
34. Lee JH, Jeong HM: Fungal sinusitis with a nasal septal perforation. Ear Nose Throat J 2013; 92(1): E24-25.