Maciej Marcinkowski, *Przemysław Ciesielski
Perianal fistula in perineal phlegmon as a complication of spontaneous rectus sheath hematoma. A case report
Przetoka okołoodbytnicza w przebiegu ropowicy krocza jako powikłanie samoistnego krwiaka pochewki mięśnia prostego brzucha – opis przypadku
Department of General Surgery, Independent Public Health Care Complex in Ostrów Mazowiecka
Streszczenie
Autorzy opisują przypadek 56-letniej pacjentki leczonej z powodu ropowicy krocza powikłanej przetokami okolicy odbytu i powierzchni przyśrodkowej uda prawego. Badania obrazowe wykazały obecność licznych zbiorników ropnych o różnych lokalizacjach, jednak nie ujawniły przyczyny powstania ropowicy i przetok. Pacjentkę zakwalifikowano do leczenia operacyjnego w trybie pilnym. Śródoperacyjnie wykluczono odkryptową etiologię przetok. Nacięto, oczyszczono i zdrenowano liczne zbiorniki ropne i przetoki skórne. Następnie kontynuowano leczenie za pomocą terapii podciśnieniowej. Zastosowane leczenie doprowadziło do zagojenia ran. Analiza retrospektywna wykazała, że najbardziej prawdopodobną przyczyną ropowicy był samoistny krwiak pochewki mięśnia prostego brzucha, który z powodu patologicznej otyłości nie dawał typowych objawów. Otyłość, cukrzyca oraz długi czas do rozpoznania doprowadziły do grawitacyjnego rozprzestrzeniania się ropowicy w obrębie krocza, pachwiny prawej i uda prawego oraz powstania przetok skórnych.
Summary
The authors present a case of a 56-year-old female patient treated due to perineal phlegmon complicated with fistulas in the anal region and medial region of the right thigh. Imaging scans demonstrated the presence of numerous pus collections at various sites, but did not reveal the cause of phlegmon and fistulas. The patient was deemed eligible for an urgent surgery. The crypt-related etiology of fistulas was ruled out intraoperatively. The numerous pus collections and cutaneous fistulas were incised, cleansed and drained. Subsequently, treatment was continued using negative pressure wound therapy. The treatment led to wound healing. The retrospective analysis demonstrated that the most probable cause of phlegmon was spontaneous rectus sheath hematoma that had an atypical manifestation due to pathological obesity. Obesity, diabetes and delayed diagnosis led to the gravitational spread of phlegmon within the perineum, right groin and right thigh, and to the formation of cutaneous fistulas.

Introduction
Rectus sheath hematoma (RSH) is a rare cause of acute abdominal pain. It is caused by blood extravasation from the epigastric vessels or their perforators, or by a tear of the rectus muscle. Hematoma is typically located in the lower abdomen. It is thrice as common in elderly women as in men at the same age (1). The factors contributing to hematoma infection are: obesity, advanced age, diabetes, steroid therapy, chronic antibiotic therapy, immune disorders, using injectable medications and psychoactive agents. Abscesses may form in an atypical course of the disease. These lesions may be spontaneously evacuated through the skin by forming fistulas that mimic crypt-related fistulas (2).
Case report
A 56-year-old patient was admitted to the Department of General Surgery on an emergency basis due to a perianal fistula and phlegmon in the perineal region and medial right thigh. At admission, the patient’s condition was moderate with fever of up to 38°C. The interview revealed pathological obesity and type 2 diabetes treated with insulin. She denied abdominal or perineal trauma. The physical examination revealed multiple, oozing external openings of fistulas over the skin of the perineum and medial region of the right thigh. Fluctuant lesions in the regions mentioned above were palpable through the integuments. Laboratory tests revealed elevated WBC (10.56 g/l) and CRP (86 mg/l). Imaging scans showed communicating collections of dense fluid in the mid hypogastric region, perineum and right thigh.
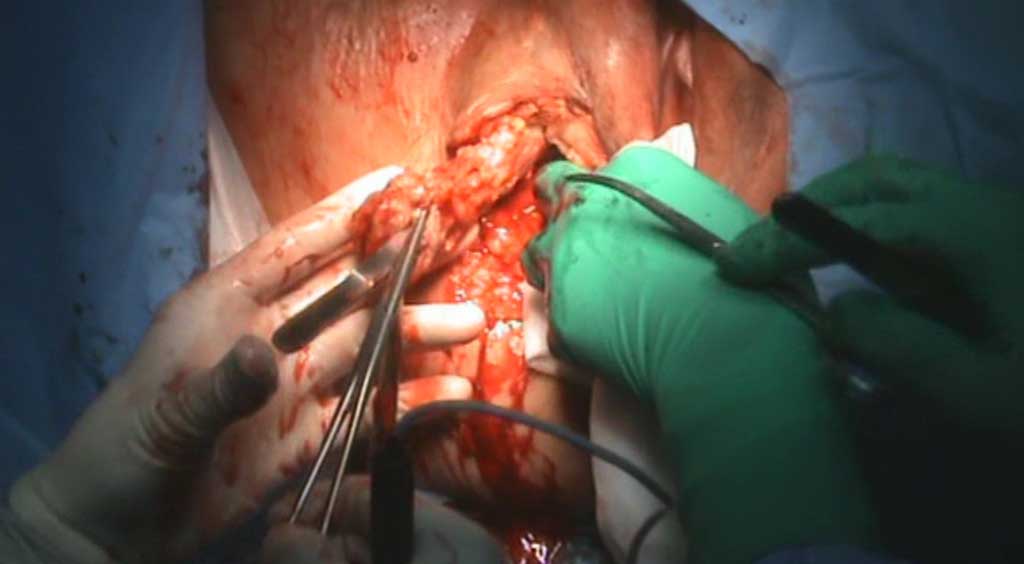
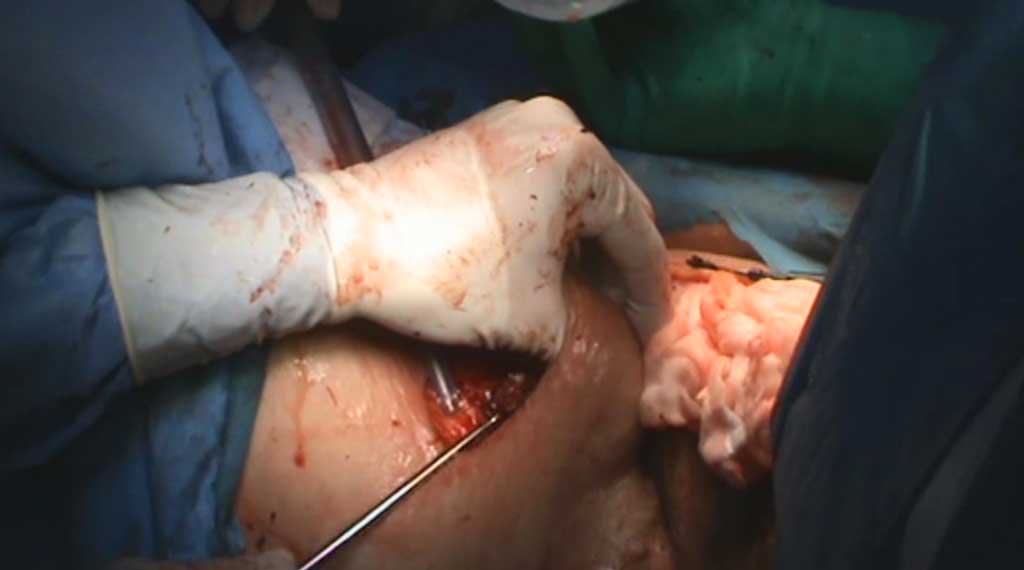
The patient was deemed eligible for an urgent surgery. In the lithotomy position, an instrumental fistula revision and rectoscopy were performed. The lesions were not communicating with the anal canal. There were two pus collections located within the right thigh, collections at both sides of the vulva and an abscess in the hypogastric region. All abscesses were opened via separate incisions. The abscess cavities contained inflammatory granulation tissue and non-foul-smelling material, typical of chronic abscesses and fistulas. Samples were collected for microbiological evaluation. Subsequently, fistulas were excised and inflamed tissue was removed to the accessible extent. The abscess beds were rinsed abundantly with sterile NaCl 0.9% solution. Setons saturated with Betadine solution were placed in the abscess beds (fig. 1-4).

Fig. 1. Excision of the fistula canal in the perineal region

Fig. 2. Curettage of the abscess bed in the hypogastric region

Fig. 3. Curettage of the abscess bed in the perineal region

Fig. 4. Status post surgery. Setons saturated with Betadine solution
In the postoperative period, empirical antibiotic therapy was applied (piperacillin with tazobactam) and 2 units of pRBCs were transfused. The culture of the material collected from the abscess bed revealed Staphylococcus aureus MSSA. The same antibiotic therapy was continued, in accordance with the antibiogram.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Shikhman A, Tuma F: Abdominal hematoma. StatPearls Publishing, Treasure Island (FL), 2008.
2. Żyluk A, Jagielski W, Szlosser Z: Martwicze zapalenie tkanek miękkich krocza imitujące ropień okołoodbytowy – opis przypadku. Pomeranian J Life Sci 2018; 64(1): 62-65.
3. Mehta NY, Copelin II EL: Abdominal Abscess. StatPearls [Internet] StatPearls Publishing, Treasure Island (FL), 2021.
4. Siu WT, Tang ChN, Law BKB et al.: Spontaneous rectus sheath hematoma. Can J Surg 2003; 46(5): 390.
5. Alla VM, Karnam SM, Kaushik M, Porter J: Spontaneus rectus Sheath Hematoma. West J Emerg Med 2010; 11(1): 76-79.
6. Szmidt J, Gruca Z, Krawczyk M et al.: Choroby powłok, sieci i przestrzeni pozaotrzewnowej. [W:] Podstawy chirurgii. Podręcznik dla lekarzy specjalizujących się w chirurgii ogólnej. Tom II. Medycyna Praktyczna 2004: 1041-1042.