© Borgis - Postępy Nauk Medycznych 9/2014, s. 648-651
*Lidia Ziółkowska, Agata Paszkowska, Wanda Kawalec
Infekcyjne zapalenie wsierdzia na zastawce mitralnej jako powikłanie w przebiegu kardiomiopatii przerostowej zawężającej – wciąż aktualny problem
Mitral valve infective endocarditis complicating hypertrophic obstructive cardiomyopathy – still a current problem
Department of Pediatric Cardiology, The Children’s Memorial Health Institute, Warszawa
Head of Department: prof. Wanda Kawalec, MD, PhD
Streszczenie
Infekcyjne zapalenie wsierdzia w przebiegu kardiomiopatii przerostowej występuje rzadko. Doniesienia piśmiennictwa zawierają głównie opisy przypadków klinicznych, dlatego też ocena stopnia ryzyka rozwoju infekcyjnego zapalenia wsierdzia u chorych z kardiomiopatią przerostową zarówno w populacji osób dorosłych, jak i u dzieci jest trudna. Przedstawiamy przypadek infekcyjnego zapalenia wsierdzia w przebiegu kardiomiopatii przerostowej ze zwężeniem drogi odpływu z lewej komory u 17-letniego chłopca, u którego proces zapalny wsierdzia doprowadził do uszkodzenia zastawki mitralnej, co wymagało pilnego leczenia kardiochirurgicznego i jej wymiany na zastawkę mechaniczną.
Summary
Infective endocarditis in the course of hypertrophic cardiomyopathy is rare. Literature reports mainly contain descriptions of clinical cases, and therefore the risk assessment of infective endocarditis in patients with hypertrophic cardiomyopathy, both in the adults and children, is difficult. We present a case of infective endocarditis in a teenage boy with obstructive hypertrophic cardiomyopathy, in which the inflammatory process has damaged mitral valve, what required an urgent cardiac surgery and mitral valve replacement with a mechanical valve.

Introduction
Infective endocarditis (IE) in the course of hypertrophic cardiomyopathy (HCM) is a rare complication, however, it is a serious therapeutic problem (1-4). According to some authors, the probability of IE in patients with HCM within 10 years is about 5% (2). The risk of endocarditis is particularly high in patients with obstruction of the left ventricular outflow tract (LVOTO) and the high value of the systolic pressure gradient in the left ventricular outflow tract (1-6). In the echocardiography bacterial vegetations are usually located on the anterior mitral valve leaflet, on the aortic valve, or both. The inflammatory process can damage the heart valves, cause of their significant regurgitation, what requires urgent cardiac surgery (1-3, 5-7).
Case Report
Currently, 17 year old boy, in whom hypertrophic obstructive cardiomyopathy was diagnosed at the age of 5 years. Since the age of 10 year, he was taken care of a pediatric cardiologist in the district center. From November 2010 (at the age of 15) the patient reported feeling worse, increasing fatigability. In December 2010, he was hospitalized in pediatric cardiology referral center, where the elevated values of inflammatory markers, thickening of the mitral valve leaflets and third degree mitral regurgitation were found. In the chest X-ray pneumonia was diagnosed, and intravenous antibiotic therapy (cefuroxime) has been applied. In January 2011 the boy was urgently admitted to the paediatric cardiology departament with fever 38 degrees, with marked dyspnoea at rest. Tachycardia 137/min, systolic murmur 3/6 scale of Levin along the left sternal border and at the apex of the heart and liver enlargement were present. In the chest X-ray bilateral parenchymal density, features of chronic congestion in the pulmonary circulation, enlarged cardiac silhouette (cardio-thoracic ratio 0.56) were found. The values of the inflammatory markers were increased, while the blood cultures obtained were negative. The antibiotics (clarithromycin and cefuroxime) have been taken for 11 days to give a slight reduction of the inflammatory markers and the alleviation of fever. In echocardiography features of hypertrophic obstructive cardiomyopathy were present: the thickness of the interventricular septum was 17.9 mm (normal values indexed to the body surface area 4.9-8.5 mm), the thickness of the left ventricle posterior wall was 11 mm (normal values corrected to the body surface area 4.3-9.5 mm), obstruction of the left ventricular outflow tract with the maximum systolic pressure gradient 100 mmHg, systolic motion of the anterior mitral leaflet and its adherence to the hypertrophied interventricular septum and the mitral valve regurgitation third degree also were found (fig. 1, 2).
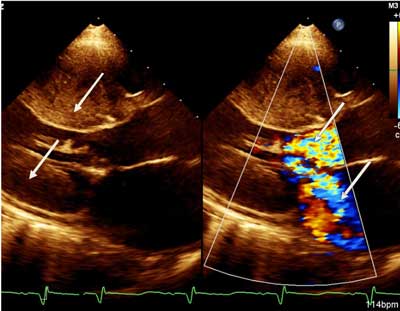
Fig. 1. Septal and left ventricular posterior wall hypertrophy, obstruction of the left ventricular outflow tract, a significant mitral regurgitation (arrows). Echocardiographic parasternal long axis view.
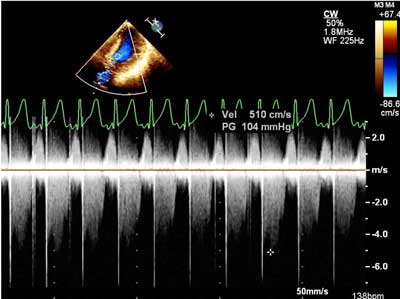
Fig. 2. Hypertrophic obstructive cardiomyopathy. Narrowing the left ventricular outflow tract with maximum systolic gradient of 104 mmHg (maximum velocity in the LVOT 510 cm/sec). Continuous wave Doppler echocardiography in the apical 5-chamber projection.
Moreover, the presence of three bacterial vegetation on the anterior mitral valve leaflet were visualised (one with a diameter of 4.5 mm moving into the left atrium, the second with a diameter of 6.2 mm at the end of the leaflet, the third of the diameter of 8mm in the middle of the leaflet) (fig. 3).
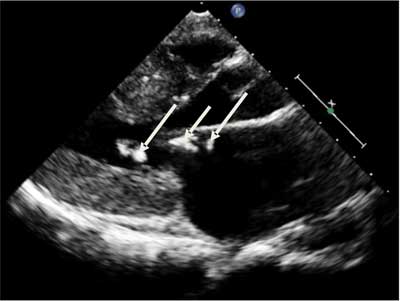
Fig. 3. Hypertrophic obstructive cardiomyopathy. Bacterial vegetations on the anterior leaflet of the mitral valve (arrow). Echocardiographic parasternal long axis view.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Noel N, Naheed Z: Hypertrophic cardiomyopathy: role of current recommendations by the American Heart Association for infective endocarditis. Pediatr Cardiol 2013; 34: 709-711.
2. Morgan-Hughes G, Motwani J: Mitral valve endocarditis in hypertrophic cardiomyopathy: case report and literature review. Heart 2002; 87: e8.
3. Spirito P, Rapezzi C, Bellone P et al.: Infective endocarditis in hypertrophic cardiomyopathy: prevalence, incidence, and indications of antibiotic prophylaxis. Circulation 1999; 99(16): 2132-2137.
4. Alessandri N, Pannarale G, del Monte F et al.: Hypertrophic obstructive cardiomyopathy and infective endocarditis: a report of seven cases and a review of the literature. Eur Heart J 1990; 11(11): 1041-1048.
5. Zhang LH, Fang LG, Yang J et al.: Infective endocarditis in patients with hypertrophic obstructive cardiomyopathy: five cases report. Chinese Journal of Cardiology 2012; 40(3): 209-213.
6. Ninomiya M, Takamoto S, Kotsuka Y et al.: Hypertrophic obstructive cardiomyopathy associated with mitral regurgitation due to infective endocarditis. The Japanese Journal of Thoracic and Cardiovascular Surgery 2000; 48(12): 820-823.
7. Roberts WC, Kishel JC, Mcintosh CL et al.: Severe mitral or aortic valve regurgitation, or both, requiring valve replacement for infective endocarditis complicating hypertrophic cardiomyopathy. JACC 1992; 19(2): 365-371.
8. Guidelines for the Prevention, Detection and Treatment of Infective Endocarditis (new version-2009). The Working Group of the European Society of Cardiology for the Prevention, Detection and Treatment of Infective Endocarditis. Eur Heart J 2009; 30: 2369-2413.
9. Maron BJ, Lever H: In defense of antimicrobial prophylaxis for prevention of infective endocarditis in patients with hyperytophic cardiomyopathy. J Am Coll Cardiol 2009; 54: 2339-2340.
10. Forner L, Larsen T, Kilian M, Holmstrup P: Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol 2006; 33: 401-407.
