Małgorzata Badełek-Izdebska, Małgorzata Dębska, *Lidia Zawadzka-Głos
Lingual tonsil hypertrophy as a cause of obstructive sleep apnea syndrome – case report
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Lidia Zawadzka-Głos, MD, PhD
Summary
The hypertrophy of the lingual tonsil (LTH) could be the cause of obstructive sleep apnea in children. This disorder may cause obstructive sleep apnea (OSA) and also may lead to a life-threatening obstruction of the upper airway. Lingual tonsil hypertrophy is more frequently described in adults. LTH often occurs in children with prior palatine tonsillectomies or adenoidectomies. Diagnosis of lingual tonsil hypertrophy in patients with OSA requires a careful ENT examination by advanced technologic methods. The sleep apnea is successfully treated by lingual tonsillectomy, with or without tracheotomy. Tracheostomy allows the obstructive airway with postoperative oedema to be bypassed.
In this study we present the case of a child with persistent syndroms of a sleep apnea. Patient underwent six adenotonsillectomies in the past. ENT examination and CT scans showed that symptoms of OSA were caused by lingual tonsil hypertrophy. Patient was treated with a lingual tonsillectomy with tracheotomy and it was an effective treatment for this case.
INTRODUCTION
The lingual tonsil, together with the palatine and pharyngeal (adenoids) tonsils, forms a Waldeyer’s ring. The lingual tonsil is a small lymphatic tissue located at the back of the base of the tongue. It’s a team cells protecting input to the respiratory and digestive systems. Being a lymphatic tissue, lingual tonsil protects against infection. The most common diseases of the lingual tonsil are tonsillitis, lingual hypertrophy and lingual tonsil cancer. Sometime the lingual tonsil become so enlarged that it obstruct the respiratory passage, leading to breathing difficulty. These hypertrophied tonsil is removed through tonsillectomy.
CASE REPORT
A 9-years-old boy was admitted to our hospital due to snoring, sleep apnea episodes and problems with swallowing. Patient underwent six operations for tonsils: in October 2005 – adenotonsillotomy and tympanotomy, in April 2006 – re-adenotonsillotomy, in May 2007 – re-adenotonsillotomy and tympanotomy, in December 2007 re-tonsillotomy and tympanotomy right ear, in February 2010 – re-adenotonsillotomy and ventilation tube of right ear, in February 2012 – re-adenotomy and lingual tonsillectomy by coblation.
On admission to our Department measured blood oxygenation was 96 to 98%. The patient in a sitting position demonstrated the lingual tonsil hypertrophy with the aid of a laryngeal mirror. A computed tomography scanning of a child’s neck revealed the airway with irregular tissular mass on the base of tongue and in region of epiglottis (fig. 1, 2).
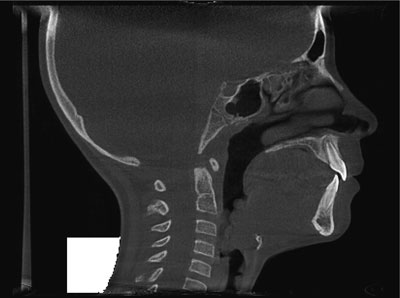
Fig. 1. CT of the enlarged lingual tonsil.

Fig. 2. CT of the enlarged lingual tonsil.
The size of the tumor was 24 mm x 20 mm. Adenoid and both palatine tonsils were non-enlarged and there were no bony deformations in this region.
The child was qualified for lingual tonsillectomy. In the evening before planned operation patient began to complain about severe pain around the right testicle. The convolution of appendix testicle was diagnosed. The child was qualified for emergency surgical treatment but the tracheal intubation was failed because of large tumorous lesions obstructing a view of the epiglottis. Rima glottidis and the vocal cords also could not be seen by an anestesiologist. The intubation via direct laryngoscopy was unsuccessful on 2 attempts. On the next day direct laryngoscopy was performed. Intubation was extremely difficult due to hypertrophic tissue at the base of the tongue. The masses from the base of tongue of enlarged lingual tonsil were removed from the laryngopharynx by the forceps and bipolar electrocautery (fig. 3).

Fig. 3. The masses on the base of tongue.
The tumor was not very well vascularized. Intraoperative histopathologic examination showed hypertrophic tonsillar tissue in the specimen. The tracheotomy was made because of high risk of upper airway and the tongue edema. Successful surgical treatment of appendix testicle convolution was done immediately after laryngological operation.
The patient after operation was nursed in an intensive care unit overnight, breathing by a tracheotomy tube. On the sixth postoperative day when supraglottic edema had resolved tracheostomy tube was removed. There was no change in clinical measurements SpO2 (98-100%). Postoperative period was uneventful and the child was discharged from hospital in 9 days. When the patient was seen 3 months later, the airway was clear and there was no evidence of obstructive sleep apnoea (OSA).
DISCUSSION
Lingual tonsil is immunological organ included in the Waldeyer’s ring. Lingual tonsil hypertrophy in children is a rarely reported disorder. The symptoms of LTH are dysphagia, sore throat, grunting, obstacles feeling in the throat, voice disturbances, chronic cough and snoring. Nocturnal symptoms are snoring, sleep pauses or breath holding and it can lead to obstructive sleep apnea syndrome (2). Diagnosis of lingual tonsil hypertrophy in patients with OSA requires a ENT examination, fiberoscopic examination, computed tomography (CT) or magnetic resonance (MR) and polisomnography (2). Enlargement of the lingual tonsil is relatively common in children with persistent obstructive sleep apnea after palatine tonsillectomy and adenoidectomy (3, 4). It is recognized that LTH also has an increased prevalence in obese children, patients with Down syndrome, and other craniofacial anomalies and there are risk factors for adenotonsillectomy failure (1, 2, 5, 6). Large lingual tonsillar hypertrophy can completely obstruct any view of the larynx during surgery and cause tracheal intubation difficult (7, 8).
Lingual tonsillectomy is an effective treatment for LTH, however perioperative airway problems should be expected. There are several different methods for resecting lingual tonsil tissue. Besides transorally tonsillectomy with direct excision are used laser, microdebrider, suction electrocautery, coblation and bipolar radiofrequency (6, 9-13). No one is the best surgical technique and the treatment of LTH is still under debate.
Lingual tonsillectomy is an effective treatment for LTH, however perioperative airway problems should be expected (8).
In this study we demonstrate that lingual tonsil hypertrophy can lead to the obstructive sleep apnea syndrome and LTH is one of important causes of renewed OSAS in patients after adenotonsillectomy (2, 5).
Piśmiennictwo
1. Chan DK, Jan TA, Koltaj PJ: Effect of obesity and medical comorbidities on outcomes after adjunct surgery for obstructive sleep apnea in cases of adenotonsillectomy failure. Arch Otolaryngol Head Neck Surg 2012 Oct; 138(10): 891-896. 2. Abdel-Aziz M, Ibrahim N, Ahmed A et al.: Lingual tonsils hypertrophy; a cause of obstructive sleep apnea in children after adenotonsillectomy: operative problems and management. Int J Pediatr Otorhinolaryngol 2011 Sep; 75(9): 1127-1131. 3. Golding-Wood DG, Whittet HB: The lingual tonsil, a neglected symptomatic structure. J Laryngol Otol 1989; 103: 922-925. 4. Enoz M, Lapeña JF: Recurrent obstructive sleep apnea due to compensatory hypertrophy of lingual tonsils following UPPP. Internet J Otorhinolaryngol 2008; 7: 1-8. 5. Guimaraes CV, Kalra M, Donnelly LF et al.: The frequency of lingual tonsil enlargement in obese children. Am J Roentgenol 2008 Apr; 190(4): 973-975. 6. Kuo CY, Parikh SR: Can lingual tonsilletomy improve persistent obstructive sleep apnea? Laryngoscope 2014 Oct; 124(10): 2211-2212. 7. Arrica M, Crawford MW: Complete upper airway obstruction after induction of anesthesia in a child with undiagnosed lingual tonsil hypertrophy. Paediatr Anaesth 2006 May; 16(5): 584-587. 8. Patel AB, Davidian E, Reebye U: Complicated airway due to unexpected lingual tonsil hypertrophy. Anesth Prog 2012 Summer; 59(2): 82-84. 9. Mowry SE, Ament M, Shapiro NL: Lingual tonsil hypertrophy causing severe dysphagia: treatment with plasma-mediated radiofrequency-based ablation (Coblation). Ear Nose Throat J 2010 Mar; 89(3): 134-136. 10. Kandoğan T, Olgun L, Ozüer MZ: Management of lingual tonsillar hypertrophy using microdebrider. Kulak Burun Bogaz Ihtis Derg 2008 Sep-Oct; 18(5): 323-325. 11. Bock JM, Trask DK: Coblation-assisted lingual tonsillectomy for dysphagia secondary to tongue base hypertrophy. Ann Otol Rhinol Laryngol 2008 Jul; 117(7): 506-509. 12. Maturo SC, Hartnick CJ: Pediatric lingual tonsillectomy. Adv Otorhinolaryngol 2012; 73: 109-111. 13. Conacher D, Meikle D, O’Brien C: Tracheostomy, lingual tonsillectomy and sleeprelated breathing disorders. Br J Anesth 2002; 88(5): 724-726.



