Monika Jabłońska-Jesionowska, *Lidia Zawadzka-Głos
Respiratory stridor in children due to congenital abnormalities of the great vessels
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Lidia Zawadzka-Głos, MD, PhD
Summary
Introduction. The respiratory stridor is a clinical symptom of airway obstruction; depending on the location of the pathology we distinguish between inspiratory, expiratory and mixed stridor. Due to the coexistence of congenital airway pathology, stridor is frequently mixed. The most common cause of congenital stenosis of the airways is laryngomalacia, followed by paralysis of the vocal cords and congenital stenosis of the cricoid cartilage. A rare but important causes of the airways narrowing in children are anomalies of the great vessels compressing the trachea and bronchi from the outside.
Aim. Aim of this study is to analyze the symptoms in children with respiratory stridor due to anomalies of the great vessels causing pressure on the respiratory tract from the outside.
Material and methods. Retrospective study involved a group of 110 children hospitalized in the Pediatric Otolaryngology Department Medical University of Warsaw in 2011-2014 years due to congenital respiratory stridor. During the diagnostics procedures following tests were made: chest X-ray, US of the larynx, US of the brain, X-ray of the esophagus with contrast, echocardiogram and laryngotracheoscopy under general anastesia, chest angio-CT, neurological and cardiac consultation.
Results. After analyzing of the cases, there has been found: laryngomalacia in 54, congenital paralysis of the vocal folds in 6, congenital stenosis of the cricoid cartilage in 5, hemangioma of the larynx in 5, laryngeal papilloma in 1, larynx cyst in 5, vascular ring in 31 cases. Identified as vascular rings include: double aortic arch –– 5 cases, right aortic arch – 6 cases, anomalies of brachiocephalic trunk – 5 cases, left aortic arch with right lusorian artery – 14 cases, pulmonary sling – 1 case. The clinical symptoms presented by children with rings: respiratory stridor, exercise stridor, silent cry, sleep apnea, cyanosis, dysphagia, recurrent infections of the inferior respiratory tract. The age of children diagnosed with vascular ring ranged from 1 week to 11 years.
Conclusions. 1. Congenital respiratory stridor always requires clinical interdisciplinary investigation. 2. Vascular anomalies are a major cause of congenital non-laryngeal respiratory stridor in children of all ages. 3. As a standard the endoscopy of the lower airways, not only the larynx but also trachea should be performed. 4. Lack of lower airways endoscopy in the diagnostic of congenital respiratory stridor can cause lack of recognition of vascular rings. 5. Deleted proper diagnosis of vascular anomalies can caused chronic changes in lower respiratory tract, weight and growth deficiency.
INTRODUCTION
Respiratory stridor is the clinical symptom and not a disease. This is the sound arised when air flows through narrowed airways. The pathology on the glottis level generates inspiratory stridor and around subglottis and trachea inspiratory-expiratory stridor (1). Airways narrowing may be due to the pathology in their interior or due to external pressure on the respiratory tract. The most common cause of congenital respiratory stridor is laryngomalacia called as congenital laxity of the larynx (2), then congenital vocal cord paralysis and congenital stenosis of the cricoid cartilage. Narrowing of the airways caused by external compression due to congenital vascular anomalies, referred as the vascular ring is very rare and is 0.7-1.3% of all congenital heart anomalies (3, 4). The ring is the result of anatomical abnormalities in the course of aorta and its branches, which cause various types of stenosis of the trachea and/or the esophagus. There are many anatomical variants of the vascular ring. The most common defect is a double aortic arch, further right aortic arch with aberrant left subclavian artery (5, 6). The clinical symptoms occur with varying intensity, depending on the degree of compression on the esophagus or the trachea in patients with vascular ring. Symptoms include: respiratory stridor, dysphagia, choking, recurrent respiratory tract infections, chronic cough (3, 5-8).
AIM
The aim of this study is to analyze the symptoms in children with respiratory stridor due to anomalies of the great vessels causing external pressure on the respiratory tract.
MATERIAL AND METHODS
In the Department of Pediatric Otolaryngology Medical University of Warsaw in 2011-2014 years 110 children were hospitalized because of an congenital respiratory stridor. During the diagnostic procedures in all children were made: perinatal anamnesis, pediatric examination, chest X-ray, larynx US and brain US, ECG and echocardiography in the case of the heart pathology in the pediatric examination, neurological examination in the case of brain US pathology. Measurement of 24 h blood oxygen saturation was control. Then in all 110 children laryngotracheoendoscopy under general anesthesia was performed. In 31 children after endoscopy chest CT angiography with contrast was performed, and in 31 children after endoscopy, barium swallow X-ray of the esophagus was performed.
RESULTS
After examining 110 children: congenital laxity of the larynx in 54 children, congenital vocal cord paralysis in 6 children, congenital stenosis of the cricoid cartilage in 5 children, hemangioma of the larynx in 4 children, laryngeal cysts in 5 children, laryngeal papilloma in 1 child, vascular ring in 31 children were recognized. The variety types of vascular anomalies were identified: a double aortic arch in 5, right aortic arch with aberrant left subclavian artery in 6, anomalies of brachiocephalic trunk in 5, left aortic arch with right lusorian artery in 14, pulmonary sling in 1. The types and number of vascular anomalies are shown in table 1.
Table 1. The types and numbers of vascular anomalies.
| Type of vascular ring | Number of children |
| A double aortic arch | 5 |
| Right aortic arch with aberrant left subclavian artery | 6 |
| Anomalies of brachiocephalic trunk | 5 |
| Left aortic arch with right artery lusoria | 14 |
| Pulmonary sling | 1 |
In the case of left aortic arch with right lusorian artery further vocal cord paralysis was diagnosed in 1 child, laryngomalacia in 2 children and partial laryngeal cleft in 1 child. In the case of right-aortic arch coexistence of defects were much more bigger (5). In 8 cases: 1 child with Fallot tetralogy, 2 children with defect in intraventricular septum, 1 child with defect in atrial septum, 1 child with interruption of the aortic arch and 1child with narrowing of the left branch of pulmonary artery were found.
Age and sex
Children who went to a clinic due to stridor ranged in age from 7 days to 11 years of age. 9 children were under the age of 1 month of age, 15 to 3 months of age, 3 at age 6-12 months, 3 at the age of 2-5 years, one at the age of 8 and one at the age of 11 years. Children with permanent respiratory stridor or silent cry reported to the clinic in the first weeks of their life.
Symptoms
Vascular ring compressing the trachea, bronchus and esophagus cause symptoms in the respiratory and digestive systems. The clinical symptoms presented by that children: respiratory stridor – 31 (100%), exercise stridor – 6 (19%), silent cry – 3 (9.7%), sleep apnea – 5 (16%), cyanosis – 1 (3.2%), dysphagia – 14 (45%), recurrent infections of the inferior respiratory tract – 12 (38.7%). All children had respiratory stridor. It was inspiratory or inspiratory-expiratory stridor. The most severe occurred in children with double aortic arch, pulmonary sling artery and anomalies of the brachiocephalic trunk and in children accompanied by defects of the larynx: vocal cord paralysis, and stenosis of the cricoid cartilage. Other symptoms in the newborn due to airway compression: apnea with observed declines in oxygen saturation, cyanosis, silent cry/weeping and cough. Older children, aged up of 12 months presented exertional dyspnoea, chest pain, decreased exercise tolerance, chronic cough. It’s necessary to pay attention to recurrent pneumonia and recurrent inflammation of the larynx and trachea. One child was treated unsuccessfully with bronchial asthma, one was diagnosed of immunodeficiency syndrome due to recurrent infections. Symptoms related to the compression on the esophagus include: choking, spitting food, excessive salivation, lack of weight gain. Choking with dysphagia occurred in 8 children with left-sided aortic arch with right subclavian artery. That artery leaves the last from the aortic arch on the left, and returned on the right side extending between the esophagus and the spine in seven cases, and between the esophagus and the trachea in one causing a narrowing of the esophagus by compression from the outside. Choking also occurred in 3 children with double aortic arch and in 5 with right aortic arch. 8 year old girl with exercise stridor, chronic cough and choking from childhood years were prescribed a diet of solid food elimination. She was treated with growth factor because of growth deficiency.
DISCUSSION
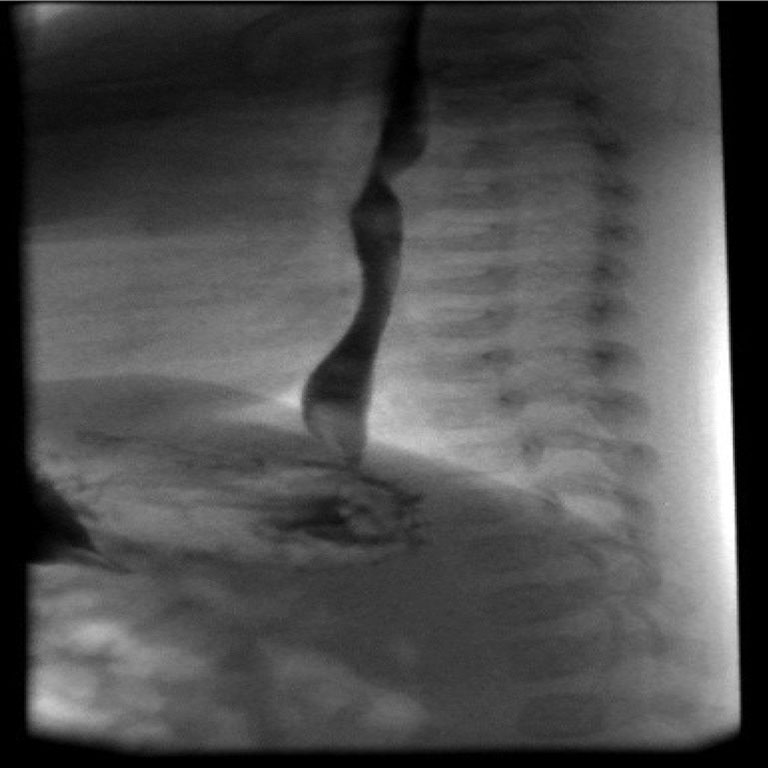
Each congenital respiratory stridor in children requires a multidisciplinary diagnostic process: laryngological, cardiological and neurological. Cardiological investigation is needed because of congenital cardiovascular pathology and neurological in cases of paralysis of the vocal cords to exclude diseases of the central and peripheral nervous system. Endoscopy under general anesthesia of the lower respiratory tract (larynx and trachea) is the standard procedure (7, 9). Out of 110 children who have been reported to the ENT Department due to stridor in 54 (49%) had laryngomalacia, which resolves spontaneously about 1.5 years old. In the remaining 56 (51%) other causes of stridor were found: laryngeal and non-laryngeal requiring an appropriate treatment (4, 9). Changes in the larynx in the form of cysts, laryngeal clefts were treated endoscopically. In the case of vocal cord paralysis procedure of laterofixation after tracheostomy was performed. Hemangiomas of the larynx were treated with oral beta-blocker to give the involution changes within 5-8 months of starting treatment. Vascular anomalies are a major non-laryngeal cause of congenital respiratory stridor in children of all ages. The assessment of the degree of airway compression during endoscopy is one of the selection criteria for cardiac surgery. In 14 children appropriate surgical treatment was performed, other children are covered periodically by a cardiologist. Lack of diagnostic process based on the assumption that the majority of congenital respiratory stridors are caused by laryngomalacia that resolves spontaneously or implementation that diagnostic on the later stage deprive children of normal development opportunities and exposes to the development of complications. The children were treated without effect due to asthma and also diagnosed with potential immune disorders due to recurrent infections. One girl was treated with growth factor because of growth disorder. Chest X-ray image is highly unspecific for the diagnosis of vascular rings. Irregularities were found only in two cases with associated congenital heart defect: tetralogy of Fallot and defect in intraventricular septum (5). An important test for the diagnosis of esophageal ring is an x-ray with barium swallow (6, 7, 9). Characteristic loss of shadow suggests a related form of the ring. In most cases, a shadow loss is at the rear of the esophagus, a front cavity is characteristic for pulmonary sling artery and non changes in anomalies of brachiocephalic trunk (fig. 1).
Fig. 1. Barium swallow X-ray – loss of shade from the back.
Echocardiography not always confirms the diagnosis of the ring, it’s limited to the child’s behavior (7). Ultimately, determining the diagnosis of vascular ring test is an angio-CT of the chest (9). It is necessary in each case for surgical intervention.
CONCLUSIONS
1. Congenital respiratory stridor always requires clinical interdisciplinary investigation.
2. Vascular anomalies are a major cause of congenital non-laryngeal respiratory stridor in children of all ages.
3. As a standard the endoscopy of the lower airways, not only the larynx but also trachea should be performed.
4. Lack of lower airways endoscopy in the diagnostic of congenital respiratory stridor can cause lack of recognition of vascular rings.
5. Deleted proper diagnosis of vascular anomalies can caused chronic changes in lower respiratory tract, weight and growth deficiency.
Piśmiennictwo
1. Zawadzka-Głos L, Zając B, Chmielik M: Stridor krtaniowy u dzieci. Magazyn Otolaryngologiczny 2005; supl. VII: 15-21. 2. Zawadzka-Głos L, Zając B, Chmielik M, Badełek-Izdebska M: Zwężenie podgłośniowe krtani w aspekcie praktycznym. Nowa Pediatria 2005; 3: 105-107. 3. Sakakura K: Congenital laryngeal anomalies presenting as chronic stridor: a retrospective study of 55 patients. Auris nasus larynx 2008 Dec; 35(4): 527-533. 4. Jabłońska-Jesionowska M, Zawadzka-Głos L: Congenital respiratory stridor in children. New Medicine 2013; 4: 120-123. 5. Woods RK, Sharp RJ, Holcomb GW et al.: Vascular anomalies and tracheoesophageal compression: a single institution’s 25-year experience. Ann Thorac Surg 2001; 72: 434-439. 6. Skalski JH, Wites M, Haponiuk I: Pierścienie naczyniowe. Rozdz. 25: 361-373. 7. Bove T, Demanet H, Casimir G et al.: Tracheobronchial compression of vascular origin. J Cardiovasc Surg 2001; 42: 663-666. 8. Saji P, Shyh-Jye Ch, Wu M-H et al.: Retroespohageal aortic arch: diagnostic and therapeutic implications of a rare vascular ring. Int J of Cardiol 2001; 79: 133-141. 9. Jeeyani HN, Prajapati VJ, Patel NH, Shah SB: Imaging features of double aortic arch shown by multidetector computed tomography angiography. Ann Pediatr Cardiol Jul-Dec 2010; 3(2): 169-170.