Jolanta Jadczyszyn, Karolina Raczkowska-Łabuda, Małgorzata Dębska-Rutkowska, *Lidia Zawadzka-Głos
Sudden bilateral deep hearing loss in a child – case study
Nagły obustronny niedosłuch w stopniu głębokim u dziecka – studium przypadku
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Associate Professor Lidia Zawadzka-Głos, MD, PhD
Streszczenie
Wstęp. Nagły obustronny niedosłuch u dziecka w stopniu głębokim jest bardzo rzadko spotykany. Szacuje się, że może występować w około 2% przypadków niedosłuchu u dzieci. Przyczyną nagłego obustronnego niedosłuchu może być ostry uraz akustyczny, zaburzenia unaczynienia ucha wewnętrznego, nagła infekcja wirusowa lub bakteryjna czy urazy ucha wewnętrznego. Hałas jest obecnie ważnym czynnikiem uszkodzenia słuchu. Grupami szczególnie narażonym na uszkodzenie zdrowia w wyniku hałasu są dzieci i młodzi dorośli. Skutkiem hałasu są różnego stopnia zaburzenia słuchu oraz coraz częściej rozpoznawane efekty pozasłuchowe w postaci uczucia niepokoju, drażliwości, zaburzeń zdolności poznawczych, obniżonej sprawności intelektualnej, utrudnionego zasypiania, zaburzeń w układzie krążenia, zaburzeń hormonalnych czy zmiany zachowań społecznych.
Opis przypadku. Zaprezentowany został przypadek 9-letniej dziewczynki, u której wystąpił nagły obustronny niedosłuch. Czynnikiem uszkadzającym słuch był głośny dźwięk dzwonka szkolnego podczas przerwy lekcyjnej. Po 6 tygodniach od wystąpienia epizodu nagłego lewostronnego niedosłuchu, dołączył się niedosłuch po stronie prawej o nieznanej etiologii. Przy przyjęciu stan ogólny dziewczynki był dobry, nie obserwowano zawrotów głowy i zaburzeń równowagi. W badaniu audiometrii tonalnej stwierdzono obustronny niedosłuch mieszany w stopniu głębokim. Leczenie w szpitalu obejmowało wykonanie zabiegu operacyjnego w postaci obustronnej tympanotomii eksploratywnej ucha środkowego z tympanocentezą przednią i obustronnym drenażem wentylacyjnym oraz leczenie zachowawcze: deksametazon, wipocentyna, piracetam, witaminy z grupy B, ksylometazolinę oraz hiperbarię tlenową. Hospitalizacja trwała 14 dni. Uzyskano całkowitą poprawę słuchu.
Wnioski. Nagły obustronny niedosłuch u dziecka w stopniu głębokim może być spowodowany ostrym urazem akustycznym. Badania wykazują, że hałas stanowi ważny czynnik uciążliwy w środowisku szkolnym i może być czynnikiem szkodliwym. Poziomy hałasu rzędu 80-85dB mierzone w korytarzach podczas przerw szkolnych i w salach gimnastycznych mogą powodować ryzyko uszkodzenia słuchu. Następstwa urazu spowodowane hałasem u dzieci są bardzo trudne do przewid
Summary
Introduction. Sudden bilateral deep hearing loss is very rare in children. Its estimated prevalence is 2% among children with hearing loss. The causes include acute acoustic trauma, vascular disorders of the inner ear, sudden viral or bacterial infection, and trauma of the inner ear. Noise is currently an important risk factor for hearing impairment. Groups that are particularly vulnerable to noise damage include children and young adults. The effects of noise include hearing impairment of different degree and the more and more commonly diagnosed extra auditory effects of noise in the form of anxiety, irritability, cognitive impairment, reduced intellectual ability, difficulty in falling asleep, circulatory disorders, hormonal disorders, and changes in social behavior.
Case report. We present a case of a 9-year-old girl who experienced sudden bilateral deep hearing loss of the left ear, which was caused by a school bell during a school break. Six weeks after the sudden hearing loss in the left ear, hearing loss in the right ear of the unknown etiology appeared. The girl was in good general condition, no vertigo and balance impairment were observed. In the tonal audiometry, bilateral deep mixed hearing loss was observed. The treatment in the hospital included surgery in the form of bilateral explorative tympanotomy of the middle ear with anterior tympanocentesis and tube insertion, as well as conservative treatment: dexamethasone, vipocentin, piracetam, B vitamins, xylometazoline, and hyperbaric oxygen therapy. Hospitalization lasted 14 days. A complete recovery of hearing was achieved.
Conclusion. Sudden bilateral deep hearing loss in children can be caused by an acute acoustic trauma. Studies show that noise is an important disturbing factor in the school environment and may be harmful. Noise levels of ca. 80-85 dB measured in corridors during school breaks and in sports halls may pose a risk of hearing impairment. The consequences of trauma caused by noise in children are very difficult to predict. It is important to recognize the problem early, as well as to introduce a proper diagnostic process and implement the treatment quickly, wh
Introduction
Sudden bilateral deep hearing loss rarely occurs in children. It is estimated that it occurs in about 2% of cases of hearing impairment (1). The etiology of the sudden bilateral hearing loss is still not fully understood. The probable factors include vascular disorders of the inner ear, infections – mostly viral, trauma of the temporal bone, and, occurring more and more often, acoustic trauma (2). Noise is one of the most oppressive harmful environmental factors, and with the civilizational progress, noise exposure has been increasing. Excessive exposure may lead to health hazards (3).
Hearing impairment may be caused by a single exposure to noise or by a long-term exposure (4). Acute acoustic trauma is caused by a noise of a very high sound pressure level that usually exceeds the threshold of pain (120-140 dB). The effect of such stimulus is a sudden (temporary or permanent) sensorineural hearing impairment, often unilateral, sometimes accompanied by tinnitus. If the structures of outer and middle ear are simultaneously affected, the hearing impairment may have a mixed character (4).
The following types of noise causing acoustic trauma can be enumerated: pure tone sound, street and industrial noise, shooting noise, and explosion (5).
The degree of hearing loss depends on the intensity of the noise, the duration of exposure on a given day, as well as lifetime exposure, the frequency of the sound, the type of the noise (intermittent, continuous, pulse), age and sex of the patient, as well as individual ear sensitivity, which is difficult to define and is probably affected by some innate features of the middle and inner ear, determining, among others, the efficacy of sound conduction, as well as the blood supply and oxygenation of the cochlea (5, 6).
The most common type of the hearing loss is the sudden unilateral sensineural hearing loss in the high frequencies with accompanying tinnitus.
Children and adolescents are considered to be particularly vulnerable to noise-induced hearing loss (4).
The risk of sudden hearing loss in children is increased by, among others, available toys (whistles, trumpets, music toys, toy guns – ca. 100-135 dB) and fireworks explosions (ca. 145-160 dB) (7). However, the biggest threat is posed by discos (92-111 dB), rock music concerts (ca. 90 dB), listening to music (ca. 86 dB), motorsports (ca. 80 dB), and shooting sports (ca. 170 dB) (8, 9).
Case report
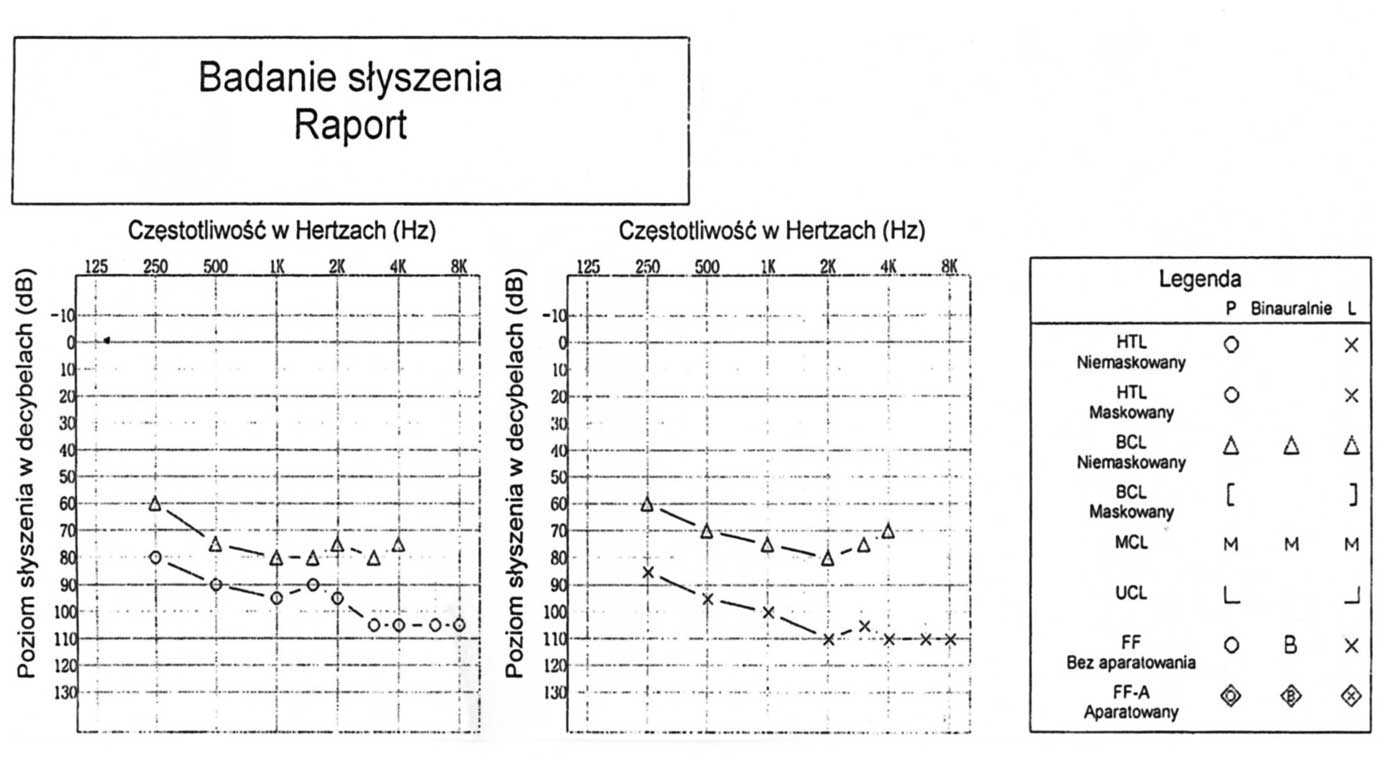
A nine-year-old girl was admitted on an emergency basis to the Department of Pediatric Laryngology of the Medical University of Warsaw because of bilateral mixed hearing loss. Approximately 6 weeks before the admission, the patient experienced an acoustic trauma in her school due to school bell ringing during school break. Since that time, she had experienced hearing impairment in her left ear, however, she had not told her parents about it. Therefore, she had not been examined by a pediatrician or a laryngologist, nor had she been referred to a hospital or received any treatment. It was only the occurrence of bilateral hearing impairment that prompted the girl’s parents to consult a laryngologist and to report to the hospital. The day before the admission, a minor viral infection of the upper respiratory tract occurred, accompanied by sudden hearing loss in the right ear. On admission in the emergency room, no findings in the general physical examination were observed – lymph nodes were not enlarged, normal vesicular sound was heard over the lungs, no arrhythmias were detected, abdominal organs were not enlarged, meningeal signs were negative. On admission to the Department of Pediatric Laryngology, the general condition of the patient was good. She did not report tinnitus or vertigo. Medical history collected from the mother included hearing loss since the day before – the girl had not been responding to commands and had been asking to repeat phrases. In the otoscopy, tympanic membranes were gray, pale, without signs of perforation, slightly drawn in the direction of the tympanic cavity, with a trace of exudate in the left tympanic cavity, without signs of acute inflammation in any of the ears. In the endoscopic examination, a minor adenoid hypertrophy was identified nasopharyngeal lumen was wide, pharyngeal openings of the auditory tubes were slightly swollen. In the hearing test: Weber was lateralized to the left ear, and in the Rinne test, the duration of air conduction was shorter than the bone conduction (Rinne negative). On tonal audiometry performed on an outpatient basis on admission, a bilateral mixed deep hearing impairment was detected (fig. 1). In the laboratory tests, no raised inflammatory markers were observed tab. 1. Due to the medical history and abnormal hearing examination, the girl was qualified for surgery on an emergency basis. In general anesthesia, explorative tympanotomy was performed and a normal ossicular chain was found, without damage to the joints and ossicles, no perilymph fistula of the inner ear was found. On the right side, the tympanic membrane was pulled into the epitympanum and overlayed the ossicular chain. On the left side. a trace amount of exudate was observed in the tympanic cavity, and the pathological secretion was removed. On both sides, 2 mg of Dexaven were administered into the tympanic cavity. Subsequently, bilateral tympanocentesis with tube insertion was performed. Conservative treatment included dexamethasone, vipocentin, piracetam, B vitamins, and xylometazoline. Due to the bilateral deep hearing loss and no signs of otitis media, it was decided to implement hyperbaric oxygen therapy. The hospitalization lasted 14 days. During the hospital stay, the patient felt well, no adverse effects of medication nor of the hyperbaric oxygen therapy were observed. The control tonal audiometry was performed after one day of treatment (fig. 2), and after 10 days of treatment (fig. 3), with satisfactory results.
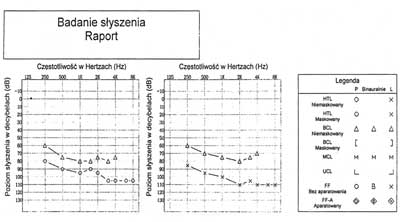
Fig. 1. Audiometry performed on the admission day
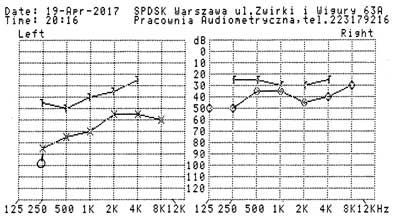
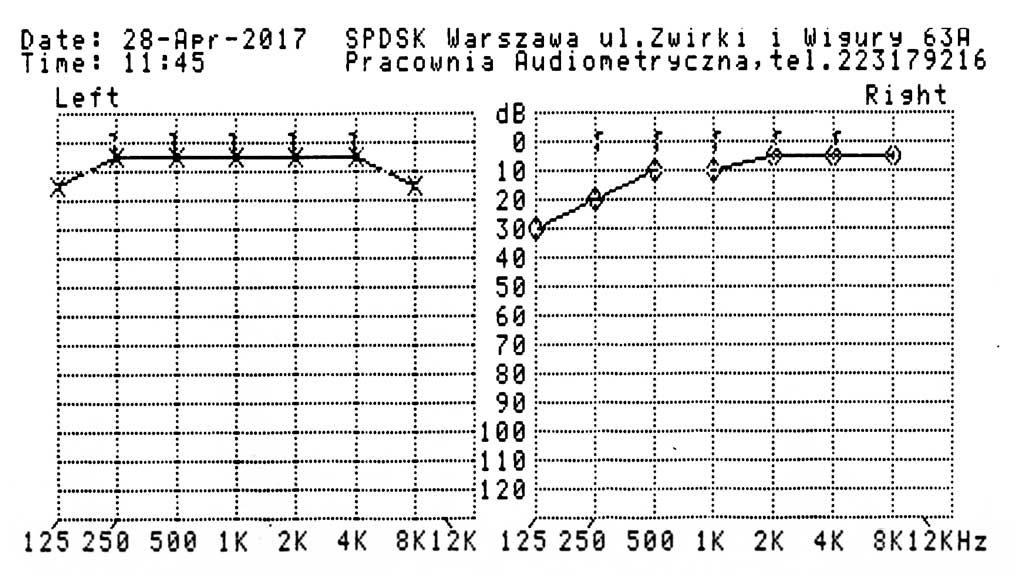
Fig. 2. Audiometry performed in the first day of treatment

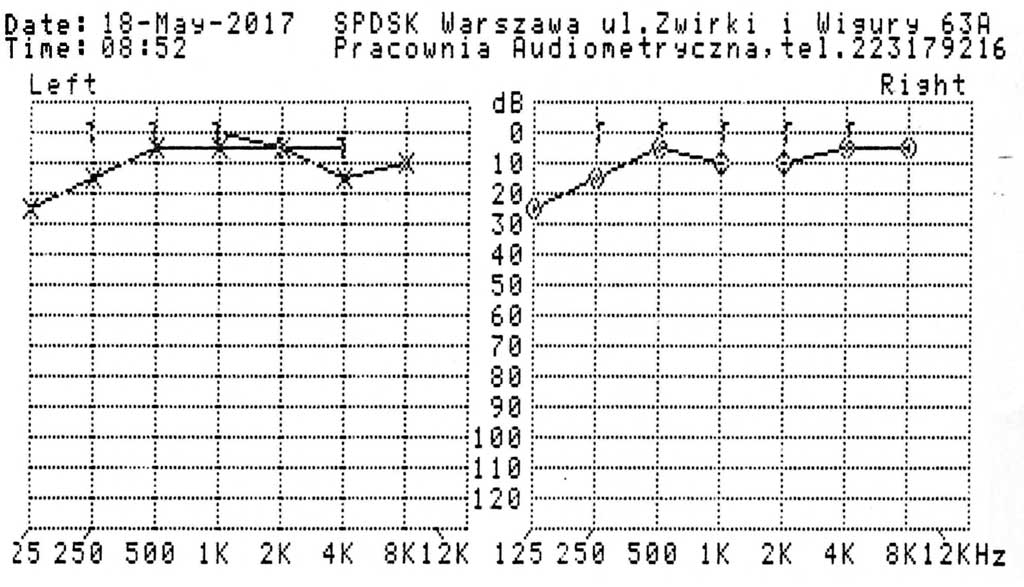
Fig. 3. Audiometry performed in the 10th day of treatment
Tab. 1. Laboratory findings on admission
| Test | Result | Reference values |
| WBC | 9.57 thousands/mL | 4.0-12.0 thousands/mL |
| RBC | 4.29 mln/mL | 4.5-5.5 mln/mL |
| HGB | 12.2 g/dL | 12-15.5 g/dL |
| PLT | 266 thousands/mL | 150-400 thousands/mL |
| Lymph % | 41% | 29.6-49.8% |
| Neut % | 46% | 43-65% |
| Mono % | 11.2% | 4.2-11.3% |
| CRP | < 0.5 mg/dL | 0-1 mg/dL |
| total calcium | 10.2mg/dL | 8.9-10.1 mg/dL |
| natrium | 142 mmol/L | 132-145 mmol/L |
| kalium | 3.7 mmol/L | 3.5-5.1 mmol/L |
| phosphorus | 4.8 mg/dL | 3.7-5.6 mg/dL |
| magnesium | 2.0 mg/dL | 1.6-2.3 mg/dL |
| INR | 1.21 | 0.9-1.25 |
| APTT | 26.67 s. | 28-40 s. |
| fibrinogen | 2.53 g/L | 1.8-3.5 g/L |
After 15 sessions of hyperbaric oxygen therapy with good tolerability, with simultaneous pharmacological treatment, a complete recovery of hearing was achieved, and the treatment was completed with very good results. Auditory examination was repeated on the outpatient basis 2 weeks after the completion of the treatment (fig. 4).

Fig. 4. Audiometry performed after the completion of the treatment
Discussion
Noise exposure is particularly high in industrialized and developing regions of the world (3, 10). The damaging effect of noise on inner ear is a result of micromechanical injury, metabolic disorders associated with oxidative stress, an excessive production of reactive oxygen species, an excessive production of glutamic acid in synaptic connections between the cells of the inner ear and afferent nerve fibers, circulatory disturbances in the stria vascularis of cochlear duct, and ionic disorders in body fluids (11-14). Although most publications on hearing impairment concern adults, the threat is not limited to people working in the industry. Recently, many clinical and epidemiological studies have indicated that children and adolescents are also in danger of an increasing exposure to noise (14, 15). The groups with particularly high risk include children treated in intensive care units, prematurely born and low-weight infants, children treated with ototoxic medications, persons that spend long time in a noisy environment, persons suffering from hearing impairment, tinnitus, hearing hypersensitivity, and persons who have positive family history of hearing impairment (10, 16). Noise may sometimes cause very serious hearing damage, often permanent, and hearing impairment has become an important social problem. It must be taken into account that extra auditory effects of noise may also occur, but are underdiagnosed due to their non-specificity. According to many authors, these effects include anxiety, irritability, fatigue, cognitive impairment and reduced intellectual ability, sleep disturbances (change of sleep phases, excessively light sleep, frequent awakenings), circulatory disorders (increased heart rate, heart palpitations, dyspnea, fatigue), disorders of the immune system, hormonal disorders, and changes in social behavior (17-20). In the case presented in this article, the girl had experienced acute acoustic trauma of the left ear caused by school bell ringing 6 weeks before the admission to the hospital. During this time, she had not reported a problem, and thus, had not been reported to a pediatrician or a laryngologist by her parents nor teachers and had not been treated. The day before the admission, an infection of the upper respiratory tract of the probably viral origin had occurred, leading to hearing loss on the right side. Only the occurrence of bilateral hearing loss had been noticed by the parents and the patient was admitted to the hospital. On tonal audiometry on the day of admission, bilateral mixed deep hearing impairment was diagnosed. The girl was qualified for bilateral explorative tympanostomy in order to examine the structures of the middle ear to diagnose the cause of the hearing loss. Due to the suspicion of impaired patency of the right auricular tube and slight exudate in the left tympanic cavity, tubes were inserted to ensure proper ventilation of the middle ear. The observed bilateral deep hearing loss was probably caused by the acute acoustic trauma caused by a school bell and perhaps also by the viral infection. The role of viral infections in children is frequently discussed in cases of sudden hearing loss, however, it is difficult to determine, as virology examinations are not frequently performed. It is believed that the most objective test would be the examination of the inner ear fluid, and that blood tests and cerebrospinal liquor may not be conclusive despite an infection (21).
Due to the noise exposition in the medical history and deep bilateral hearing loss, hyperbaric oxygen therapy (HBO) was also included in the treatment plan. Indications for HBO are based on the results of experimental studies and clinical trials on physiological, physical and biochemical effects of exposure to hyperbaric oxygen therapy (22). Hyperbaric oxygen therapy is defined by UHMS (Undersea and Hyperbaric Medical Society) as an intervention in which an individual breathes 100% oxygen intermittently while inside a hyperbaric chamber that is pressurized to greater than sea level pressure (1 atmosphere absolute, or ATA) (23). The therapeutical effects of hyperbaric oxygen therapy remain a subject of scientific debate and research. In literature, there are numerous reports of side effects of hyperbaric oxygen therapy, including impaired patency of pharyngotympanic tube, feeling of fullness in the middle ear, and exudative otitis media, which may require tube insertion in some cases (24). In addition, cases of myopia, seizures, tympanic membrane perforation, tinnitus, vertigo, and, in case of pregnant women, also fetal complications, are described in the literature (25). In the case presented in this article, no auricular complications have been observed, thanks to the bilateral tube insertion before the beginning of the hyperbaric oxygen therapy. It must be also taken into account that one-sided hearing impairment in children is often unnoticed by them and they may not report any problem for a long time. In the case presented in this paper, the patient had not visited a pediatrician or a laryngologist for 6 weeks after the trauma had occurred. Only the occurence of hearing impairment in the right ear and consequent bilateral hearing impairment prompted the parents of the child to seek help urgently. Often it is the long-term complications, such as school problems, attention deficits, concentration problems, requirement for frequent repetition, and repetition of words and phrases, that suggest the problem to the parents or teachers (26, 27). It must also be considered that the contact with a child may be limited, as the child may marginalize the problem or not be able to name the symptoms. Therefore, in the era of constantly increasing noise intensity, early education of both children and parents is of primary importance. Hearing impairment caused by noise results in many complications, not only associated with physical health, but also social, emotional, intellectual, and linguistic problems. The world has become a noisy place and a threat to all of us, including our children. Excessive noise level in schools related to the student’s activities during school breaks and during physical education lessons in the sports halls, as well as outside noises, not only cause hearing impairment, but may also negatively affect learning process, concentration, attention, speech perception and general health condition (28). According to the results of some studies, about 10-20% of all the teenagers and young adults under 18 years of age are at risk of hearing loss and tinnitus as a result of voluntary listening to loud music using personal CD and MP3 players, participating in mass events, such as music festivals, concerts, and discos (29-31). Hearing impairment has become a problem so serious that WHO (World Health Organization) has issued a report on the occurrence of the disorder in the world. According to this report, there are 360 million people with hearing impairment around the world, of which 32 million (9%) are children (32). Moreover, WHO notes that as many as 1.1 billion young people worldwide may be at risk of hearing loss (32).
It is therefore essential to continuously take effective, comprehensive actions, implement age-targeted educational programs for students of primary and secondary schools, as well as their parents and teachers, in order to familiarize them with potentially harmful noise sources in the environment.
Conclusions
1. Sudden bilateral hearing loss rarely occurs in children.
2. The noise of considerable intensity occurring in nurseries, kindergartens, and schools can cause hearing impairment.
3. The occurrence of sudden hearing loss may be preceded by the symptoms of an acute viral infection.
4. The consequences of hearing loss in children are difficult to predict. It is important to recognize the problem early, to introduce a proper diagnostic process and implement the treatment quickly, which is a key to the positive outcome.
5. Oxygen therapy and hyperbaric oxygen therapy have their indications and contraindications, and their use is associated with the possibility of complications.
6. Prophylaxis, aiming at reducing the impact of harmful environmental risk factors for acoustic trauma, is important.
Piśmiennictwo
1. Byl FM: Sudden hearing loss: eight years experience and suggested prognostic table. Laryngoscope 1984; 94: 647-661.
2. Rogowski M: Nagła głuchota. In: Śliwińska-Kowalska M (eds.): Audiologia Kliniczna. 1st Edition, Łódź: Mediton Oficyna Wydawnicza; 2005. 263-269.
3. Choi SH, Choi CH: Noise-induced neural degeneration and therapeutic effect of antioxidant drugs. J Audiol Otol 2015; 19: 111-119.
4. Śliwińska-Kowalska M: Uszkodzenia słuchu spowodowane hałasem. In: Śliwińska-Kowalska M (eds.): Audiologia Kliniczna. 1st Edition: Łódź: Mediton Oficyna Wydawnicza; 2005. 289-298.
5. Szmeja Z: Uraz akustyczny. In: Pruszewicz A, Obrębowski A (eds.): Audiologia kliniczna. 4th Edition, Poznań: Wydawnictwo Naukowe Uniwersytetu Medycznego im. K. Marcinkowskiego; 2010. 384-400.
6. Sułkowski W, Szymczak W, Kowalska S, Sward-Matyja M: Epidemiology of occupational noise-induced hearing loss in Poland. Otolaryngol Pol 2004; 58: 233-236.
7. Plontke S, Zenner HP: Current aspects of hearing loss from occupational and leisure noise. Environmental and Occupational Health Disorders. GMS Curr Top Otorhinolaryngol Head Neck Surg 2004; 3: 233-325.
8. Bogoch II: Perceptions about hearing protection and noise-induced hearing loss of attendees of rock concerts. Can J Public Health 2005; 96: 69-72.
9. Chung JH: Evaluation of noise-induced hearing loss in young people using a web-based survey technique. Pediatrics 2005; 115: 861-867.
10. Thakur N, Batra P, Gupta P: Noise as a health hazard for children: time to make a noise about it. Indian Pediatrics 2016; 53: 111-114.
11. Henderson D, Bielefeld EC, Harris KC, Hu BH: The role of oxidative stress in noise-induced heating loss. Ear Hear 2006; 27: 1-19.
12. Falasca V, Greco A, Ralli M: Noise induced hearing loss: the role of oxidative stress. Otolaryngol Open J 2017; 5: 1-5.
13. Harrison RV: The prevention of noise induced hearing loss in children. Int J Ped 2012; 6: 1-13.
14. Sułkowski W: Uszkodzenia słuchu spowodowane hałasem u dzieci i młodzieży: przyczyny i prewencja. Med Pr 2009; 60: 513-517.
15. Carvalho WB, Pedreira ML, Aguiar MALD: Noise level in a pediatric intensiva care unit. J Pediatr 2005; 81: 495-498.
16. Ministerstwo Zdrowia Departament Zdrowia Publicznego. Seminarium dotyczące ochrony przed hałasem; https://www.mos.gov.pl/g2/big/2012_12.
17. Evans GW, Lepore SJ: Nonauditory Effects of Noise on Children: A Critical Review. Child Environ 1993; 10: 31-51.
18. Stansfeld SA, Matheson MP: Noise pollution: non-auditory effects on health. British Medical Bulletin 2003; 68: 243-257.
19. Passchier-Vermeer W, Passchier WF: Noise exposure and public health. Environmental Health Perspect 2000; 108 (suppl. 1): 123-131.
20. Lamm K, Lamm H, Arnold W: Effect of Hyperbaric Oxygen Therapy in Comparison to Conventional or Placebo Therapy or No Treatment in Idiopatic Sudden Hearing Loss, Acoustic Trauma, Niose-Induced Hearing Loss and Tinnitus. Hyperb Oxyg Ther Otorhinolaryng 1998; 54: 86-99.
21. Garcia Berrocal JR, Ramirez-Camacho R, Portero F, Vargas JA: Role of viral and Mycoplasma pneumonia infection in idiopathic sudden sensorineural hearing loss. Acta Otolaryngol 2000; 120: 835-839.
22. Hampson NB: Hyperbaric Oxygen Therapy. Committee report. Kensington MD, Undersea and Hyperbaric Medical Society 1999.
23. Fernau JL, Hirsch BE, Derkay C et al. Hyperbaric oxygen therapy: effect on middle ear and eustachian tube function. Laryngoscope 1992; 102: 48-52.
24. Gill AL, Bell CAN: Hyperbaric oxygen: its uses, mechanisms of action and outcomes. Int J Med 2004; 97: 385-395.
25. Brookhouser PE, Worthington DW, Kelly WJ: Unilateral hearing loss in children. Laryngoscope 1991; 101: 1264-1272.
26. Lieu JEC, Tye-Murray N, Karzon RK, Piccirillo JF: Unilateral Hearing Loss is Associated with worse speech-language scores in children. Pediatrics 2010; 125: 1348-1355.
27. Cunningham J, Nicol T, Zecker SG et al.: Neurobiologic responses to speech in noise in children with learning problems: deficits and strategies for improvement. Clin Neurophys 2001; 112: 758-767.
28. Passchieer-Vermeer W: Pop-music through headphones and hearing loss. Noise Control Eng J 1999; 47: 182-187.
29. Mercier V, Luy D, Hohmann BW: The sound exposure of the audience at a music festival. Noise Health 2003; 5: 51-58.
30. Daniel E: Noise and heating loss: a review. J Sch Health 2007; 77: 225-231.
31. WHO global estimates on prevalence of hearing loss. http://www.who.int/pdb/deafness/WHO_GE_HL.pdf (accessed: 2016.01.09).
32. WHO. Regional Office for Europe. CEHAPE: Children’s Environment and Health Action Plan for Europe http://www.euro.who.int./ecehrome.