© Borgis - New Medicine 1/2001, s. 22-26
Zofia Rajtar-Leontiew1, Radoslaw Kuszyk2
Haemorrhage into the adrenal glands in the neonate
1Department of Neonatal Pathology, the Medical University of Warsaw
Head: Zofia Rajtar-Leontiew
2Department of Radiology and USG Clinical Hospital, the Medical University of Warsaw
Head: Andrzej Koczynski
Summary
The authors describe the specificity of haemorrhages into the adrenal glands in the neonatal period.
Foetal adrenal glands are large in size; in the first weeks of life they are larger than the kidneys. In the second half of gestation the glands undergo a rapid involution and in a full-term neonate they are merely 1/3 of the normal kidney length. After birth their size continues to decrease swiftly with a simultaneous development of function (5).
The structure and the function of the adrenal medulla and cortex differ but the intra-adrenal glycocorticoid level may affect the conversion of norepinephrine into epinephrine. Glycocorticoids may exert their effect on the N-methyl-phenyl-ethanolamine enzyme level which is linked with the conversion. So far it has not been clearly stated how both adrenal glands affect each other, and diseases, particularly those of the adrenal medulla in foetal and neonatal life, are very rarely diagnosed (7).
The adrenal cortex secretes three main groups of hormones:
1. glycocorticoids - hydrocortisone is the most important of those and has the greatest effect on the metabolism of carbohydrates, proteins and fats;
2. mineralocorticoids - aldosterone and desoxycorticosterone affect water and mineral balance, mainly by promoting sodium retention and exchange of hydrogen ions for potassium in the distal renal canaliculi;
3. adrenal androgens - dehydroandrosterone, androstedion, and 11-B-hydroxyandrostendion in neonates are responsible for protein anabolism, and also for the type of pubic hair, mainly in girls at puberty.
The adrenal medulla secretes physiologically active catecholamines into the bloodstream, such as dopamine, noradrenaline and adrenaline, which have a potent effect on the circulatory system, the release of liver glucose and fatty acids - Catecholamine metabolites - vanillylmandelic acid (VAM), metaadrenaline and noradrenaline - are excreted into urine and may be determined for diagnostic reasons.
Anatomic and physiological abnormalities of the adrenal glands may affect only one of them, rarely both (only 10%) (7).
Haemorrhage into the adrenal glands resulting from a complicated labour, bleeding tendency or hypoxia, is a specific injury which may be associated with acute endocrine disorders which are life-threatening to the neonate (adrenal crisis).
Before the introduction of new imaging techniques such as ultrasonography (USG), computerised tomography (CT), and magnetic resonance (MRI), haemorrhage into the adrenal glands had been diagnosed very rarely, mainly at postmortem examination (3). In both old and new paediatric textbooks, haemorrhage into the adrenal glands in neonates as the primary cause of adrenal insufficiency is listed last, after congenital adrenal hyperplasia, immune and infectious disorders and neoplasia. In textbooks on neonatal endocrine disorders, hypotension and shock associated with haemorrhage into the adrenal glands, occurring in the perinatal period, are also dealt with marginally, although they are included among life-threatening causes in the neonate. Neither international nor Polish literature include reports which would present a more updated approach, despite the fact than an increasing number of abdominal and renal USG scans show evidence of haemorrhage into the adrenal glands and calcification varying in size and severity whose location is compatible with the adrenal glands.
Reported cases of calcification are associated mainly with one adrenal gland, and very rarely both. They are differentiated with calcification in the course of meconium and ileitis nauroblastoma, teratoma, and congenital Wolman´s syndrome. A small or merely one-sided haemorrhage into the adrenal glands generally does not lead to acute adrenal insufficiency. A large or moderate haemorrhage may be masked by other severe neonatal diseases: sepsis with shock, CNS injury, asphyxia, intestinal obstruction and/or atresia, pulmonary hypertension, severe anaemia, or circulatory insufficiency, because their clinical manifestations are not specific only for adrenal injury damage. In severely damaged adrenal glands there is a dramatic onset of hypovolaemic shock, hypotension, abnormal thermoregulation, carbohydrate metabolism and water and mineral imbalace, tachycardia, arrhythmia, and cyanosis. Anorexia and rapid weight loss are present. Hypoglycaemia is difficult to treat and may be accompanied by convulsions. Ion disturbances include decreased serum concentration of sodium, chlorine, occasionally calcium, and an increased concetration of potassium. Similar clinical manifestations and ion disturbances may occur in CNS injury in the neonate, mainly that of the hypthalamus and/or pituitary gland, these being the organs centrally controlling adrenal homeostasis. Diagnosis to confirm acute adrenal insufficiency is difficult, particularly when the symptoms in the neonate are life-threatening and are an indication for intensive therapeutic measures including administration of adrenal preparations.
Therefore, the neonate must undergo planned immediate investigations in order to detect possible haemorrhage into the internal organs, congenital defects and infections. The urgently required treatment should not delay differential diagnoses (2).
Additional difficulties in assessing hormonal disturbances in the neonate arise from unsTable concentrations of particular adrenal hormones for at least the first 5 days of age. This is common for both full-term and preterm newborns, especially those with a birth weight below 1500 g (6).
The most common investigations include USG examination of the head and abdomen, radiological examination of the chest, blood test, platelet count, coagulation test, blood gases, ionogram, glucose determination, blood, CFS and urine culture, infection indexes e.g., reactive protein C (CRP), granulocytic elastase, and ECG, or echocardiography and constant evaluation of the blood pressure. In order to differentiate the disease with adrenogenital syndrome and its types, assessment of adrenal hormones in the serum and a 24-hour collection of urine should be planned, depending on the newborn´s age.
It is particularly useful to assess plasma rennin activity (PRA), 17-hydroxyprogesterone (17-OHP), hydrocortisone and ACTH; the measurements can be done using immunoradometric and fluorometric techniques (6). Respective blood and urine determinations of VAM, dopamine, adrenaline and noradrenaline provide a functional assessment of the adrenal medulla, and, in association with urography, CT and MRI, facilitate a differential diagnosis of e.g., neuroblastoma.
A certain number of fatalities among the newborn in the course of shock, collapse, hyponatraemia and hypercaliaemia may be due to a complete or partial pituitary aplasia and/or brain hypoplasia, or its secondary damage. Not stimulated by control centres, the adrenal glands do not function, adequately, which, secondarily, leads to a disturbed ACTH concentration (feedback). The early neonatal period may also reveal the presence of familial Addison´s disease, described by Shepard et al. in 1959 (8). The patients show hydrocortisone deficiency and do not respond to ATCH stimulation, which, according to Migeon, is suggestive of a congenital ACTH receptor defect (4). The neonates with the syndrome present with shock, hypoglycaemia, and hyperpigmentation of the skin.
Aggravation of symptoms in the disease with age shows that it is rather a progressing degenerative process and not a congenital one. Not all cases of acute adrenal insufficiency are accompanied by shock, and the disease does not always have to develop fully. However, the disease has a very severe course when haemorrhage into the adrenal glands occurs and prognosis is not certain.
Below we present two cases treated in our Department.
Case 1
N.C. (ref. no. 4759/158/95/F), a female infant, the product of a second pregnancy, was born spontaneously at 41 weeks of gestation with an Apgar score 9 and a body weight of 3220 g. The labour lasted 3 hours and 20 min. The immediate postnatal period was uneventful. Within 48 hours she developed projectile vomiting, and abdominal distension. Due to a presumed gastrointestinal obstruction breast feeding was stopped, intravenous fluids were given, and the patient was referred to our Department for further diagnosis and treatment.
On admission the patient´s cardiovascular and respiratory systems were normal; pulse rate 120/min; respiratory rate 34/min; blood pressure normal; meconium had been passed, peristalsis was normal, but the abdomen was markedly distended. Radiological examination did not show any evidence of gastrointestinal obstruction. Glucose concentration 41.3 mg%, sodium 138 mEq/l, potassium 5.9 mEq/l, calcium 1.11 mEq/l, total bilirubin 16 mg%, urea 40%, blood pH 7.55, paO 13.6, HCO 20, BE 5.3 mEq/l, BTA negative, CRP/++, CSF normal. Urine normal. Ht 54%, RBC 5600000, WBC 19,200, rods 1, segmented 63, acidphilic 5, lymphocytes 25, monocytes 5%.
Echocardiography revealed a left-to-right shunt via a patent foramen ovale (PFO). At that time the patient was treated with adequately adjusted intravenous fluids; glucose and calcium concentrations were controlled, phototherapy was given, blood gases were normalised and oral feeding was restored. After a 3-day course of treatment abdominal distension and the patient´s anxiety subsided; bilirubin decreased to a normal level. At 4 days of age the USG examination showed a large, tumour-like, solid mass of a low echogenicity at the site of the right adrenal gland. The contour of the abnormal adrenal gland was regular, smooth and it was 40x35x25 mm size. The upper pole of the right kidney was compressed. The middle and lower part of the adrenal gland were normal. The left kidney and adrenal gland were normal. The calyces and renal pelvises and the urinary bladder were normal (fig. 1a and b).
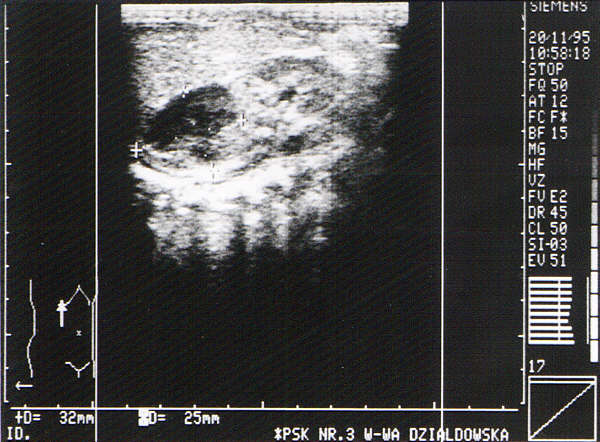
Fig. 1a and b. USG examination: a low-echogenicity tumour ca 40x35x25 mm in the right adrenal gland. The upper renal pole has been compressed by the lesion.
The examination did not exclude a likely adrenal tumour on the right side. Therefore, at the age of 6 days urography was performed, which showed that the right kidney was displaced by approximately 2 cm downward by a structure superior to its upper pole (fig. 2).

Fig. 2. Urography: the right kidney displaced downwards by a tumour-like enlarged adrenal gland. No calcification is present over the tumour.
A repeat USG examination done on the same day raised a suspicion about a haematoma in the right adrenal gland.
Further differential diagnosis of the lesion done at the age of 21 days by means of a CT scan (fig. 3) provided the final diagnosis of a haematoma in the right adrenal gland with a newly started calcification of its capsule. Normal results of VAM and adrenal metabolites excluded an active adrenal tumour.
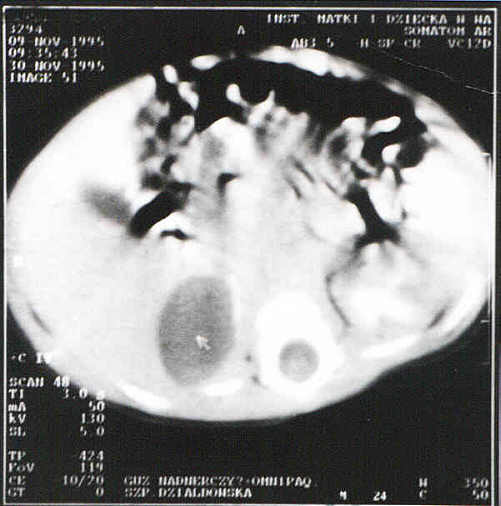
Fig. 3. CT: an encapsulated oval mass with a regular contour in the right adrenal gland dense 36jH. with microcalcifications in the wall - an adrenal haematoma.
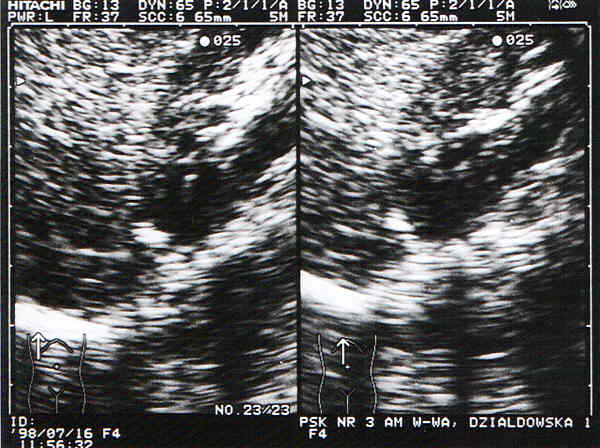
Fig. 4. USG examination (follow-up after 2 years). The adrenal gland has decreased to its normal size. Its central part shows a small, highly echogenic area with an acoustic shadow below - compatible with calcification.

Fig. 5. Plain X-ray of the abdomen (follow-up after 2 years). A small, comma-like calcification in the right adrenal gland - remission of haematoma.
On completion of the diagnostic studies it was possible to assess that the clinical manifestations found in the patient were associated with an adrenal haematoma. Their severity was not life-threatening due to the fact that the other adrenal gland compensated for impaired homeostasis. The treatment in that case was sapring, symptomatic and short-term.
With an endocrine crisis, the treatment is usually intensive and the following measures are taken:
1. glycocorticoids as life-saving agents. Mostly, hydrocortisone is given intravenously in divided doses;
2. albumins, plasma or blood and physiological salt with glucose for at least 24 hours;
3. when vasodilators are required, they should be preceded by hydrocortisone if the treatment is going to be efficient;
4. antibiotics are given until an adequate therapy is administered.
Case 2
A.W. (ref. no 2403/95/92) was the product of a second complicated pregnancy (a cervical suture from 18 weeks of gestation: mother, para 2, after iodine therapy) born at term, with an Apgar score of 7 and a body weight of 3400 g. Four hours after birth the patient´s condition exacerbated, he became pale, his limbs were cold and moist. He was given 8% intravenous glucose for presumed hypoglycaemia. At 2-3 min after the treatment was initiated, he developed shock and intravenous hydrocortisone was given followed by 5% albumins in adequately calculated doses. After 12 hours of observation and treatment with antibiotics, the patients was suspected of an intrapublic infection for which he was transferred to our Department.
On admission the newborn showed signs of disturbed peripheral circulation, had a sucking reflex but refused to suck milk from the mother´s breast or the bottle. Occasionally he had tachycardia, BP was normal. Serum glucose concentration was normal at 75-80 mg%, potassium was at the upper normal limit 5.6 mEq/l, sodium 138 mEq/l, urea initially was 53 mg% and decreased to 32 mg%. The maternal and the newborn´s blood groups were the same O Rh(+). The newborn rapidly became anaemic: at 1 day of age haemoglobin value decreased to 11.4 g%, and at 2 days it fell to 10.2 g%, and at 10 days of age it was 8.8 g%. Simultaneously, RBC decreased from 3 170 000 to 2 700 000. The USG examination of the head showed normal brain structures, and that of the abdomen revealed an abnormal mass over the left adrenal gland with increased echogenicity which was present on subsequent USG examinations. Urography done at 7 days of age, showed a slight displacement of the left kidney downwards and obliquely by a tumour-like enlarged adrenal gland (fig. 6), and CT revealed a haematoma in the left adrenal gland (fig. 7).

Fig. 6. Urography: the left kidney displaced slightly downwards and obliquely by a tumour-like enlarged left adrenal gland. No calcification present over the gland.

Fig. 7. CT: oval mass with a regular contour, Ca. 30 mm in diameter, in the left adrenal gland. Low Resolution of the lesion (dense 41, j.H.). No calcification. Haematoma in the left adrenal gland.
A 24-hour urine collection done at 12 days of age showed the following values: adrenaline 0.6 mg/day, noradrenaline 1.3 mg/day (n = 2.8-17.5 mg/day), dopamine 66 mg/day, 17-ketosteroids 0.5 ng/day and 17-OHCS-0.7 ng/day. Apart from a low adrenaline level, the results were within the normal limits for the patient´s age.
When the patient´s anaemia was the greatest, i.e. at 10 days of age, it was the second time the patient showed symptoms of a developing shock, which was immediately controlled by administration of intravenous fluids, hydrocortisone and blood transfusion. Further development of the patient was normal.
Piśmiennictwo
1. Caffey´s: Pediatric X-Ray Diagnosis, 8th edition, Silverman F Year Book Medic Publ Chicago 1985:1740:41. 2. Kruger C, Hoper K, Weissortel R, et al.: Value of direct measurement of active renin concentration in congenital adrenal hyperplasia due to 21-hydrolase deficiency. Eur J Pediatr 1966, 155, 858-61. 3. Marcinski A: Ultrasonografia pediatryczna, Warszawa 1994, Sandomedia. 4. Migeon C, Kenny E, Kowarski A, et al.: The syndrome of congenital adrenocortical unresponsiveness to ACTH, Pediatr Res 1968, 2:501. 5. Romer TE: Zaburzenia hormonalne u dzieci i mlodziezy, Warszawa 1993, Omnitech Press. 6. Saad Al Saedi, Dean H, Williams D, et al.: Screening for congenital adrenal hyperplasia: the delfia screening test overestimates serum 17-hydroxyprogesterone in preterm infants. Pediatrics 1996, 97, 1:100. 7. Shaffer-Averys: Diseases of the Newborn 1993, Vi ed. Saunders Comp Philadel, London, Toronto. 8. Shepard T, Landing B, Mason D: Familial Addison´s Disease, Am J Dis Child 1959, 97:154.
