*Patrycja Pawluszewicz, Pawel Wojciak, Inna Diemieszczyk, Piotr Golaszewski, Paulina Wozniewska, Hady Razak Hady
Hiatal hernia – epidemiology, pathogenesis, diagnostic
Przepukliny przeponowe – epidemiologia, patogeneza, diagnostyka
Ist Department of General and Endocrine Surgery, Medical University of Bialystok, Poland
Streszczenie
Przepuklina rozworu przełykowego jest częstą patologią, a częstość występowania rośnie wraz z wiekiem. Spowodowana jest wzrostem ciśnienia śródbrzusznego oraz osłabieniem tkanek odnóg przepony. Wyróżniamy przepuklinę wślizgową i przepuklinę okołoprzełykową. Pacjenci z przepukliną przeponową mają wiele niespecyficznych objawów, które sprawiają, że pacjenci leczeni są z powodu innych chorób, opóźniając właściwe leczenie. Najczęściej chorzy demonstrują objawy refluksu żołądkowo-przełykowego i leczeni są zachowawczo inhibitorami pompy protonowej.
Przeanalizowano epidemiologię występowania przepuklin rozworu przełykowego, ich patogenezę, symptomatologię, najczęściej stosowane metody diagnostyczne oraz możliwości terapeutyczne.
Rodzaj podjętego leczenia musi być dostosowany do wielkości i rodzaju przepukliny, objawów przedoperacyjnych i chorób współistniejących oraz oparte na najnowszych doniesieniach naukowych. Leczenie chirurgiczne daje dobre efekty terapeutyczne i wiąże się z niskim ryzykiem.
Summary
Hiatal hernia is a common pathology in the field of surgery, the frequency of occurrence increases along with age. It is caused by an increase anintra-abdominal pressure and weakening of the diaphragm crura tissues. Sliding hiatal hernia and paraoesophageal hernia are distinguished. Patients with diaphragmatic hernia reveal many non-specific symptoms which causes delay of proper treatment in favors of the treatment due to other diseases. The most frequently, patients present symptoms of gastroesophageal reflux and are treated conservatively with proton pump inhibitors.
Epidemiology of hiatal hernia occurrence has been analyzed along with their pathogenesis, symptomatology, the most frequently used diagnostic methods and therapeutic possibilities.
The type of applied procedure should depend on the size and type of hernia, preoperative symptoms and co-morbidities and current scientific reports. Surgical treatment brings satisfying therapeutic results and is connected with law risk of complications.

Introduction
Hiatal hernia is a frequent pathology and its frequency of occurrence increases along with age. Four types are distinguished: sliding hiatal hernia, paraoesophageal hernia, mixed hiatal hernia and giant hiatal hernia. The first is the most frequent and is connected with reflux disease (1).
Patients with hiatal hernia present many different symptoms, such as thoracic pain, dyspnea, belching, heartburn, recurrent pneumonia, hoarseness, chronic cough, anemia caused by iron deficits. Non-specific symptoms are connected with the fact that patients are under control of different specialists and are treated due to different conditions such as asthma, COPD, circulatory failure, angina, ulcerous disease (2). The most frequently, patients present symptoms of gastroesophageal reflux and are treated conservatively with proton pump inhibitors.
Literature reports that hiatal hernia coexisting with GERD brings better treatment results, lower number of remissions, higher improvement of quality of life after laparoscopic Nissen fundoplication than after conservative treatment with proton pump inhibitors. Surgical treatment is necessary in case of sliding hiatal hernia with reflux disease and paraoesophageal hernia. However, perioperative risk should be considered for patients in advanced age and numerous co-morbidities when treatment with proton pomp inhibitors brings relief. In patients with non-symptomatic hiatal hernia, the operative risk should be compared with the risk of perioperative complications (3).
The first report on hiatal hernias has been published in 1853 by Bowditch (4). Hirsch in 1900, diagnosed hiatal hernia using X-ray (5). Akerlund in 1926 proposed the term hiatal hernia and classified its 3 types which are used until now (6).
Review
Epidemiology
The frequency of occurrence of hiatal hernia increases along with age. Actual frequency of occurrence of hiatal hernia may only be estimated due to the fact that it brings only mild or no symptoms, and diagnostic criteria may differ. Clinical estimations report that approximately 50-60% of patients over 50 years old suffer from hiatal hernia (7, 8). The frequency of occurrence of symptomatic cases of hiatal hernia is strictly connected with the recognition of gastroesophageal reflux disease (GERD) due to the fact that both those conditions are strongly correlated (9, 10). Approximately 9% of hiatal hernias are symptomatic. Precise frequency of treated cases of GERD in large populations is difficult to verify but specific indexes for Western countries is within 10-20% (11-13).
Sliding hiatal hernia (type I) are significantly more frequent and consist of 90-95% of cases, esophageal type (type II) consists of only 5% where LES remains below the diaphragm and the stomach is relocated to the thorax.
Hiatal hernias occur the most frequently in highly developed countries of Northern America and Western Europe, and the most rarely in African and Eastern populations (14, 15). Some authors suggest that predispositions for hiatal hernia development include insufficient amount of fiber and high sitting position during defecation (16, 17).
Pathogenesis
Hiatal hernia may be congenital or acquired. Among acquired hiatal hernias, traumatic and nontraumatic are distinguished. The most common types of hernia are acquired in non-traumatic manner. Nontraumatic acquired hernias are divided into four subtypes: sliding (type I) and paraoesophageal (type II). Mixed type with coexisting features of sliding and paraoesophageal hernia are also observed (type III). IV type of hiatal hernia is connected with short esophagus.
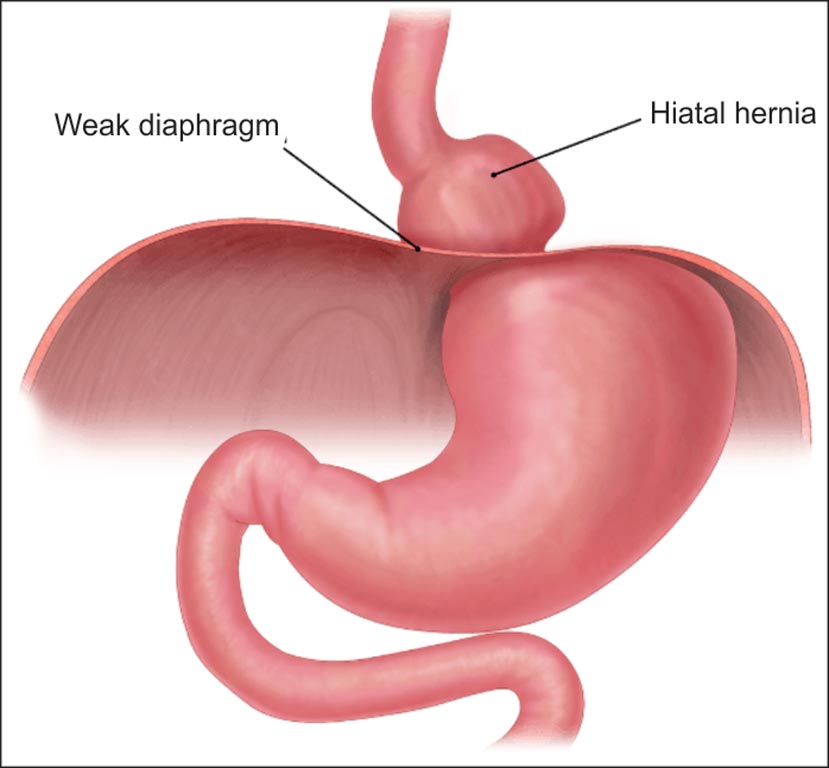
Sliding hiatal hernia is most common type of hiatal hernia. It occurs when the gastro-esophageal junction, along with the part of the stomach, migrates to the mediastinum through the esophagus (fig. 1). In the majority of patients with esophageal hernia, no symptoms are observed, in part of patients’ symptoms of reflux are visible. This type of hernia interferes with the anti-reflux barrier mechanisms in several ways. The lower esophageal sphincter (LES) relocates from an area with positive pressure inside the abdominal cavity to the area of low pressure in the thorax, which interferes with the activity of the sphincter. What is more, the relaxation of diaphragm crura reduces the anti-reflux barrier of the esophagus. The Hiss angle is lost in the diaphragmatic hernia, which causes higher risk of regurgitation of gastric contents. These changes, not only predispose to reflux of gastric contents to the esophagus, but also prolong the time of acid contact with the esophageal epithelium causing chronic esophagitis, metaplasia of the epithelium.
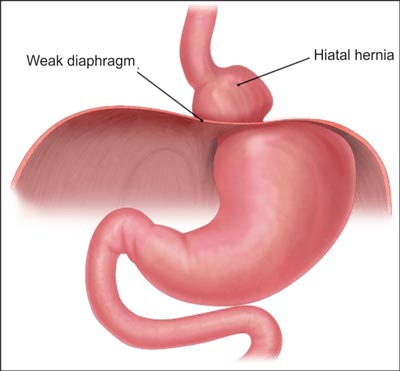
Fig. 1. Sliding hiatal hernia. Original Artwork by: https://mexicobariatriccenter.com/hiatal-hernia-paraesophageal-peh/
In the paraoesophageal hernia, broadened diaphragmatic hiatus allow to relocate the stomach fundus to the thorax, the gastro-esophageal junction stays below the diaphragm (fig. 2). Within the time, the part of the stomach and other abdominal organs moved to the thorax are enlarged. In this type of hernia, the anatomical Hiss angle remains unchanged, so there is no gastro-esophageal reflux (18).
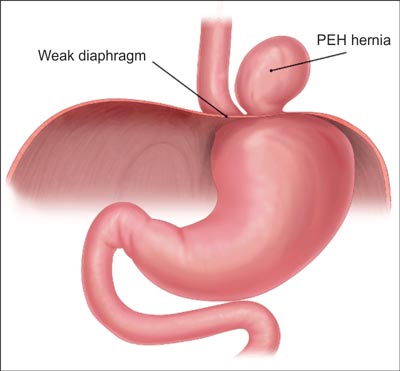
Fig. 2. Paraoesophageal hiatal hernia. Original Artwork by: https://mexicobariatriccenter.com/hiatal-hernia-paraesophageal-peh/
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Hyun JJ, Bak Y-T: Clinical significance of hiatal hernia. Gut and Liver 2011; 5(3): 267-277.
2. Mackiewicz A,Wojtun S, Gil J: Noncardiac chest pain. Pediatr Med Rodz 2013; 9(1): 25-31.
3. Korzonek M, Dziergas A, Kuczynska M: Gastroesophageal reflux disease – current problem. Forum Med Rodz 2014; 8(5): 201-210.
4. Bowditch HI: A treatise on diaphragmatic hernia. Jewettthomas, Buffalo 1853.
5. Schwarz GS: Historical aspects of the anatomy of the cardia with special reference to hiatus hernia. Bull N Y Acad Med 1967; 43: 112-125.
6. Akerlund A, Onnell H, Key E: Hernia diaphragmatica hiatus oesophageivomanastomischen und roentgenologischengesichtspunkt. Acta Radiol 1926; 6: 3-22.
7. Goyal Raj K: Chapter 286. Diseases of the Esophagus. Harrison's Principles of Internal Medicine. McGraw Hill Medical, New York 2008.
8. Mittal RK: Hiatal hernia: myth or reality? Am J Med 1997; 103: 33S-39S.
9. Skinner DB: Pathophysiology of gastroesophageal reflux. Ann Surg 1985; 202: 546-556.
10. Petersen H, Johannessen T, Sandvik AK et al.: Relationship between endoscopic hiatus hernia and gastroesophageal reflux symptoms. Scand J Gastroenterol 1991; 26: 921-926.
11. Des B, Varannes S, Marek L et al.: Gastroesophageal reflux disease in primary care. Prevalence, epidemiology and quality of life of patients. Gastroenterol Clin Biol 2006; 30: 364-370.
12. Dent J, El-Serag HB, Wallander MA et al.: Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 2005; 54(5): 710-717.
13. Spechler SJ: Epidemiology and natural history of gastro-oesophageal reflux disease. Digestion 1992; 51 (suppl. 1): 24-29.
14. Chang CS, Poon SK, Lien HC et al.: The incidence of reflux esophagitis among the Chinese. Am J Gastroenterol 1997; 92: 668-671.
15. Fujimoto K: Review article: prevalence and epidemiology of gastro-oesophageal reflux disease in Japan. Aliment Pharmacol Ther 2004; 20 (suppl. 8): 5-8.
16. Burkitt DP: Hiatus hernia: is it preventable? Am J Clin Nutr 1981; 34(3): 428-431.
17. Sontag S: Defining GERD. Yale J Biol Med 1999; 72(2-3): 69-80.
18. Polomsky M, Peters JH, Schwartz SI: Hiatal hernia and disorders of the spine: a historical perspective. Dis Esophagus 2012; 25(5): 367-372.
19. Burkitt DP, James PA: Low-residue diets and hiatus hernia. Lancet 1973; 2(7821): 128-130.
20. Sihvo EI, Salo JA, Rasanen JV et al.: Fatal complications of adult paraesophageal hernia: a population-based study. J Thorac Cardiovasc Surg 2009; 137(2): 419-424.
21. Larusson HJ, Zingg U, Hahnloser D et al.: Predictive factors for morbidity and mortality in patients undergoing laparoscopic paraesophageal hernia repair: age, ASA score and operation type influence morbidity. World J Surg 2009; 33(5): 980-985.
22. Szelachowski P, Strutynska-Karpinska M, Grabowski K et al.: Massive hiatal hernia-presentation of one case. Adv Clin Exp Med 2006; 15(2): 389-391.
23. Fernandez MC, Diaz M, Lopez F et al.: Cardiac complications after laparoscopic large hiatal hernia repair. Is it related with staple fixation of the mesh? Report of three cases. Ann Med Surg (Lond) 2015; 4(4): 395-398.
24. Banks M: The modern investigation and management of gastro-oesophageal reflux disease(GERD). Clinical Medicine 2009; 6(9): 600-604.
25. Lin S, Brasseur JG, Pouderoux P et al.: The phrenic ampulla: distal esophagus or potential hiatal hernia? Am J Physiol 1995; 268(2 Pt 1): G320-G327.
26. Kahrilas PJ: Hiatus hernia causes reflux: fact or fiction? Gullet 1993; 3(1 suppl.): 21-30.
27. Dodds WJ, Walter B: Cannon Lecture: current concepts of esophageal motor function-clinical implications for radiology. AJR Am J Roentgenol 1977; 128: 549-561.
28. Ott DJ, Gelfand DW, Chen YM et al.: Predictive relationship of hiatal hernia to reflux esophagitis. Gastrointest Radiol 1985; 10: 317-320.
29. Bytzer P: Information bias in endoscopic assessment. Am J Gastroenterol 2007; 102: 1585-1587.
30. Johnson LF, Demeester TR, Haggitt RC: Endoscopic signs for gastroesophageal reflux objectively evaluated. Gastrointest Endosc 1976; 22: 151-155.
31. Gyawali CP, Kahrilas PJ, Savarino E et al.: Modern diagnosis of GERD: the Lyon Consensus. Gut 2018; 67: 1351-1362.
32. Ott DJ, Glauser SJ, Ledbetter MS et al.: Association of hiatal hernia and gastroesophageal reflux: correlation between presence and size of hiatal hernia and 24-hour ph monitoring of the esophagus. Am J Roentgenol 1995; 165: 557-559.
33. Weijenborg PW, van Hoeij FB, Smout AJ et al.: Accuracy of hiatal hernia detection with esophageal high-resolution manometry. Neurogastroenterol Motil 2015; 27(2): 293-299.
34. Gray DM, Kushnir V, Kalra G et al.: Cameron Lesions in Patients with Hiatal Hernias: Prevalence, Presentation, and Treatment Outcome. Dis Esophagus 2015; 28(5): 448-452.
35. Stylopoulos N, Rattner DW: The History of Hiatal Hernia Surgery: From Bowditch to Laparoscopy. Annals of Surgery 2005; 241(1): 185-193.
36. Migaczewski M, Grzesiak-Kuik A, Pedziwiatr M et al.: Laparoscopic treatment of type III and IV hiatal hernia – authors’ experience. Videosurger Miniinv 2014; 2: 157-163.
37. DeMeester TR, Peters JH: Surgical treatment of gastroesophageal reflux disease. [In:] Castell DO (ed.): The Esophagus. Mass, Little, Brown and Company, Boston 1995: 577-617.
38. Petersen LF, McChesney SL, Daly SC et al.: Permanent mesh results in long-term symptom improvement and patient satisfaction without increasing adverse outcomes in hiatal hernia repair. Am J Surg 2014; 207(3): 445-448.
39. Hazebroek EJ, Leibman S, Smith GS: Erosion of a composite PTFE/ePTFE mesh after hiatal hernia repair. Surg Laparosc Endosc Percutan Tech 2009; 19(2): 175-177.
40. Soricelli E, Basso N, Genco A et al.: Long-term results of hiatal hernia mesh repair and antireflux laparoscopic surgery. Surg Endosc 2009; 23(11): 2499-2504.