Hady Razak Hady1, *Piotr Golaszewski1, Paulina Wozniewska1, Maria Soldatow2, Jacek Lapinski2, Mikolaj Czerniawski1, Inna Diemieszczyk1, Lukasz Szarpak3, Jacek Dadan1, Jerzy Robert Ladny1, 4
Surgical treatment of incisional hernia – own material
Postępowanie chirurgiczne w leczeniu przepuklin pooperacyjnych – materiał własny
1Ist Department of General and Endocrine Surgery, University Clinical Hospital in Bialystok, Poland
2Surgery Department, Independent Public Health Care Center, Lapy, Poland
3Lazarski University, Warsaw, Poland
4Department of Emergency Medicine, Medical University of Bialystok, Poland
Streszczenie
Wstęp. Przepukliny pooperacyjne stanowią częste odległe powikłanie zabiegów przeprowadzanych w obrębie jamy brzusznej. Powstanie przepukliny zależy od czynników związanych ze stanem ogólnym pacjenta oraz techniką przeprowadzania zabiegu. Jedyną formą leczenia przepuklin pooperacyjnych jest zabieg naprawczy.
Cel pracy. Celem pracy było przedstawienie i analiza doświadczeń własnych w leczeniu przepuklin pooperacyjnych. Operacje przeprowadzono w I Klinice Chirurgii Ogólnej i Endokrynologicznej w Białymstoku oraz na Oddziale Chirurgii Ogólnej Samodzielnego Publicznego Zakładu Opieki Zdrowotnej w Łapach.
Materiał i metody. Do badania zakwalifikowano 146 chorych: 65 kobiet i 81 mężczyzn. Średnia wieku chorych wynosiła 61,5 roku. Warunkiem włączenia do badania była obecność przepukliny pooperacyjnej. Analizie poddano następujące czynniki: rodzaj pierwotnej operacji, przyczyny powstania przepukliny, objawy kliniczne, choroby towarzyszące oraz zastosowany zabieg naprawczy.
Wyniki. Wśród kobiet objętych badaniem najczęstszym pierwotnym zabiegiem było cięcie cesarskie, a wśród mężczyzn appendektomia. Większość pacjentów jako główną dolegliwość podawała wystający worek przepuklinowy oraz ból okolicy przepukliny pojawiający się podczas wysiłku. Do najczęstszych chorób współistniejących należały schorzenia układu oddechowego oraz choroby nowotworowe. Chorzy zostali poddani zabiegowi naprawczemu zarówno sposobem klasycznym, jak i laparoskopowym.
Wnioski. W patogenezie powikłań pooperacyjnych oprócz techniki chirurgicznej istotną rolę odgrywają stan kliniczny chorego oraz choroby współistniejące. Zabiegi małoinwazyjne stanowią ważny i korzystny dla chorego sposób leczenia przepuklin pachwinowych. Zapewniają mniejszą częstość infekcji miejscowych, lepsze gojenie ran pooperacyjnych oraz szybszy powrót do aktywności fizycznej oraz zawodowej.
Summary
Introduction. Postoperative hernias are frequent long-term complication of surgical procedures carried out within the abdominal cavity. Hernia occurrence depends on patient general condition and surgical technique. The only one type of incisional hernia treatment is surgery.
Aim. The aim of the study was to present and analysis personal experiences in the treatment of postoperative hernias. Operations were carried out in Ist Department of General and Endocrine Surgery, University Hospital in Bialystok and the Surgery Department at the Independent Public Health Care Center in Lapy.
Material and methods. 146 patients were included to the research, 61 women and 81 men. The mean age of examined patients was 61.5 years. Factors taken into consideration were: primary operation, the causes of the hernia, clinical symptoms, comorbidities and corrective operation.
Results. Cesarean section was the most common primary intervention in group of women, appendectomy was dominant in the group of men. The majority of patients as the main complaint gave the protruding hernia sac and the pain of the hernia area appearing during exercise. The most common comorbidities were respiratory and neoplastic diseases. Patients underwent remedial treatment both in the classic and laparoscopic way.
Conclusions. In the pathogenesis of postoperative complications, apart from surgical technique, patient general condition and coexisting diseases also play an important role. Minimally invasive procedures are an important and beneficial way of treating inguinal hernia. They provide lower incidence of local infections, better healing of post-operative wounds, faster return to daily and professional activity.

Introduction
Incisional hernias are classified as long-term complications of abdominal surgeries. Their incidence ranges from 9 to 20% (1, 2). Incisional hernias are most often located in place of the scar after a median laparotomy. Main causes of this complication are improper postoperative wound healing and states associated with elevated intra-abdominal pressure. Ventral hernias are usually asymptomatic. Patients often complain about sac protrusion (which grows with increased intra-abdominal pressure), discomfort as well as esthetic problems (3). Clinical image change in the moment of complications appearance. Hernia incarceration is manifested by severe abdominal pain, followed by symptoms of gastrointestinal obstruction. Surgery is the only way to repair the defect. Conservative treatment is ineffective. In some cases, hernia complications can develop and they need urgent surgery (4).
Aim
The aim of the study was to present personal experiences in the treatment of postoperative hernia. Operations were carried out in Ist Department of General and Endocrine Surgery, University Hospital in Bialystok and the Surgery Department at the Independent Public Health Care Center in Lapy.
Material and methods
Patient operated due to incisional hernias between 2012 and 2017 were included in the research. 85% of the patients underwent primary operation in the regional surgery departments of the Podlasie Province. Patient were operated because of emergency and elective reasons. The main condition of inclusion to the study were patients with incisional hernia. Endpoint of the research was hernioplasty.
Retrospective analysis of collected data has been conducted. Factors taken into consideration were: age, gender, clinical symptoms, the factor initiating the development of the disease, comorbidities, primary operation, type of the hernioplasty. Simple statistical methods have been used for analysis.
Results
A total of 146 patients underwent incisional hernia repair. The study population consisted of 65 women and 81 men. The youngest patient was 45 years old, the oldest was 82 years old. The mean age of examined patients was 61.5 years, 63.5 for women and 59.5 for men.
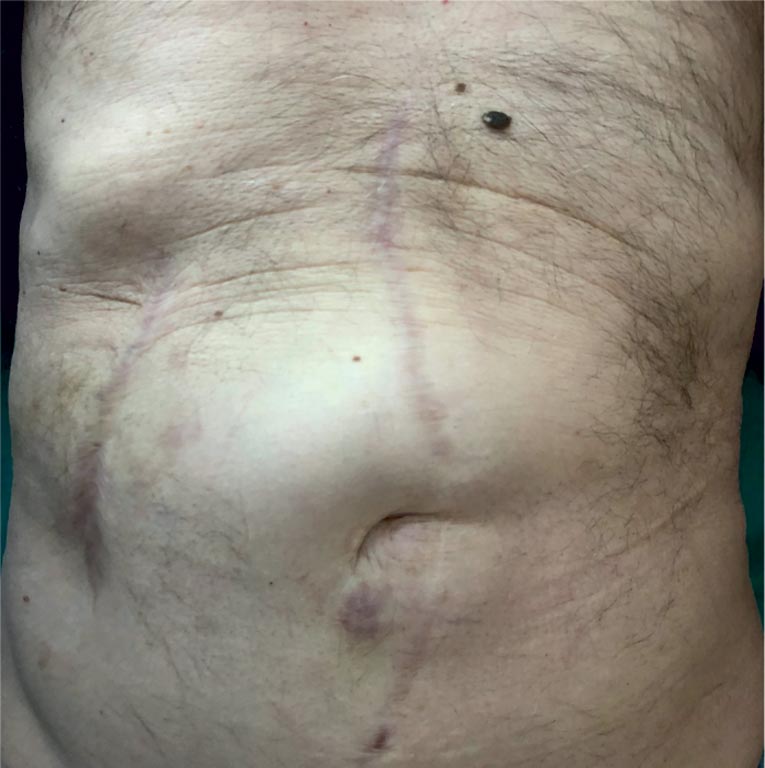
The most common patient complaints, of both women and men were protruding hernia sac (women: n51, 78.5%; men: n64, 79%), and exertional pain (women: n39, 60%, men: n50, 61.7%) (fig. 1, 2). Patients were less likely to complain about gastrointestinal track incarceration symptoms (women: n9, 13.8%, men: n7, 8.6%). The remaining symptoms included: resting discomfort, exertional discomfort, resting pain, recurrent partial gastrointestinal tract obstruction (tab. 1).
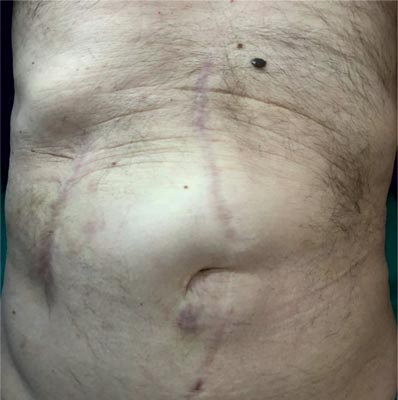
Fig. 1. Incisional hernia after right-sided hemicolectomy

Fig. 2. Incisional hernia after sleeve gastrectomy
Tab. 1. Incisional hernia – clinical characteristics
| | Women (w) n = 65 | Men (m)
n = 81 | General n = 146 |
| n | % | n | % | n | % |
| Resting discomfort | 21 | 32.3 | 30 | 37 | 51 | 35 |
| Exertional discomfort | 29 | 44.6 | 21 | 26 | 50 | 34.3 |
| Resting pain | 11 | 17 | 19 | 23.5 | 30 | 20.5 |
| Exertional pain | 39 | 60 | 50 | 61.7 | 89 | 61 |
| Protruding hernia sac | 51 | 78.5 | 64 | 79 | 115 | 78.8 |
| Recurrent partial gastrointestinal tract obstruction | 12 | 12.3 | 16 | 19.7 | 28 | 19 |
| Gastrointestinal tract incarceration | 9 | 13.8 | 7 | 8.6 | 16 | 11 |
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Van’t Riet M, Steyerberg EW, Nellensteyn J et al.: Meta-analysis of techniques for closure of midline abdominal incisions. Br J Surg 2002; 89: 1350-1356.
2. Fortelny RH, Baumann P, Thasler WE et al.: Effect of suture technique on the occurrence of incisional hernia after elective midline abdominal wall closure: study protocol for a randomized controlled trial. Trials 2015; 16: 52.
3. Ah-kee EY, Kallachil T, O’Dwyer PJ: Patient Awareness and Symptoms From an Incisional Hernia. Int Surg 2014; 99(3): 241-246.
4. Verhelst J, Timmermans L, van de Velde M et al.: Watchful waiting in incisional hernia: is it safe? Surgery 2015; 157(2): 297-303.
5. Murray BW, Cipher DJ, Pham T et al.: The impact of surgical site infection on the development of incisional hernia and small bowel obstruction in colorectal surgery. Am J Surg 2011; 202(5): 558-560.
6. Schreinemacher MH, Vijgen GH, Dagnelie PC et al.: Incisional hernias in temporary stoma wounds: a cohort study. Arch Surg 2011; 146: 94-99.
7. De Raet J, Delvaux G, Haentjens P et al.: Waist circumference is an independent risk factor for the development of parastomal hernia after permanent colostomy. Dis Colon Rectum 2008; 51: 1806-1809.
8. Caglià P, Tracia A, Borz? L et al.: Incisional hernia in the elderly: risk factors and clinical considerations. Int J Surg 2014; 12: 164-169.
9. Sørensen LT, Hemmingsen UB, Kirkeby LT et al.: Smoking Is a Risk Factor for Incisional Hernia. Arch Surg 2005; 140(2): 119-123.
10. Al Chalabi H, Larkin J, Mehigan B et al.: A systematic review of laparoscopic versus open abdominal incisional hernia repair, with meta-analysis of randomized controlled trials. Int J Surg 2015; 20: 65-74.
11. Froylich D, Segal M, Weinstein A et al.: Laparoscopic versus open ventral hernia repair in obese patients: a long-term follow-up. Surg Endosc 2016; 30(2): 670-675.
12. Eker HH, Hansson BME, Buunen M et al.: Laparoscopic vs Open Incisional Hernia Repair A Randomized Clinical Trial. JAMA Surg 2013; 148(3): 259-263.
13. Burger JWA, Luijendijk RW, Hop WCJ et al.: Long-term Follow-up of a Randomized Controlled Trial of Suture Versus Mesh Repair of Incisional Hernia. Ann Surg 2004; 240(4): 578-585.
14. Sugerman HJ, Kellum JM Jr, Reines HD et al.: Greater risk of incisional hernia with morbidly obese than steroid-dependent patients and low recurrence with prefascial polypropylene mesh. Am J Surg 1996; 171(1): 80-84.
15. Rastegarpour A, Cheung M, Vardhan M et al.: Surgical mesh for ventral incisional hernia repairs: Understanding mesh design. Plast Surg (Oakv) 2016; 24(1): 41-50.
16. Bilsel Y, Abci I: The search for ideal hernia repair; mesh materials and types. Int J Surg 2012; 10(6): 317-321.
17. Darehzereshki A, Goldfarb M, Zehetner J et al.: Biologic versus nonbiologic mesh in ventral hernia repair: a systematic review and meta-analysis. World J Surg 2014; 38(1): 40-50.