*Piotr Golaszewski1, Paulina Wozniewska1, Justyna Dawidowska2, Patrycja Pawluszewicz1, Maria Soldatow2, Martyna Wyszynska1, Hady Razak Hady1
Incisional hernia – clinical characteristics, diagnosis and treatment
Przepukliny pooperacyjne – obraz kliniczny, diagnostyka i leczenie
1Ist Department of General and Endocrine Surgery, University Clinical Hospital in Bialystok, Poland
2Pediatric Department of Pro-Medica Hospital in Elk, Poland
Streszczenie
Przepukliny pooperacyjne zaliczamy do odległych powikłań zabiegów operacyjnych przeprowadzanych w obrębie jamy brzusznej. Częstość ich występowania szacuje się na około 20%.
Przepukliny w bliźnie pooperacyjnej zajmują szczególne miejsce w chirurgii jamy brzusznej ze względu na dużą częstość występowania oraz nawrotowość. European Hernia Society (EHS) zaleca klasyfikację przepuklin pooperacyjnych w oparciu o: charakter przepukliny (pierwotna/nawrotowa), lokalizację, wielkość oraz czynniki ryzyka nawrotu schorzenia. W literaturze możemy odnaleźć wiele czynników sprzyjających powstawaniu przepuklin, m.in. choroby współistniejące upośledzające gojenie ran pooperacyjnych, stany przebiegające z podwyższonym ciśnieniem wewnątrzbrzusznym, nieprawidłowa technika chirurgiczna. Objawami, na które zwracają uwagę autorzy publikacji, są: ból, dolegliwości natury kosmetycznej (wystający worek przepuklinowy) i uczucie dyskomfortu. Jedyną skuteczną metodą leczenia jest zabieg naprawczy. Istnieje kilka technik plastyki przepuklin pooperacyjnych. Opracowania naukowe wykazują wyższą skuteczność operacji z użyciem siatek nad zabiegami polegającymi na samym zszyciu wrót przepukliny. Niniejszy artykuł zawiera przegląd danych oraz piśmiennictwa na temat epidemiologii, patogenezy, obrazu klinicznego oraz leczenia przepuklin pachwinowych.
Summary
Postoperative hernias are long-term complications of surgical procedures performed within the abdominal cavity. Their incidence is estimated at around 20%.
Postoperative hernia hold a special place in abdominal surgery due to the high incidence and recurrence. The European Hernia Society (EHS) recommends the classification of postoperative hernia based on: the character of hernia (primary/relapsing), location, size and risk factors for relapse. The available literature indicates many factors leading to the development of hernia, including co-morbidities that impair postoperative wound healing, diseases with elevated intraabdominal pressure or improper surgical techniques. The symptoms of postoperative hernias include pain, cosmetic defect (protruding hernia sac) and discomfort. The only effective way of postoperative hernia treatment is reconstructive surgery, that includes several repair techniques. Scientific studies show a higher efficacy of mesh repair methods over procedures based on tension suture techniques.
The following article contains an overview of data and literature on epidemiology, pathogenesis, clinical charactristic and treatment of incisional hernia.

INTRODUCTION
Postoperative hernias are a frequent and costs generating complication of surgical procedures performed within the abdominal cavity (1). According to the European Hernia Society (EHS) postoperative hernias should be considered as any space in the abdominal wall accompanied by or without a bulge, perceptible or palpable on examination, detected by imaging studies within the postoperative scar (2, 3). This complication applies to both operations performed using classical and laparoscopic techniques.
REVIEW
Epidemiology
The incidence of hernias depends largely on the location of the surgical incision, experience of the surgeon and the type and scope of the operation being performed. Postoperative hernias are most often located in place of the scar after a median laparotomy. Studies show a wide discrepancy in the incidence of postoperative hernia. This complication may occur in 9 to 20% of operations performed in the abdominal cavity (4, 5). More than half of hernias in the postoperative scar is diagnosed within the first year after surgery (6).
Classification
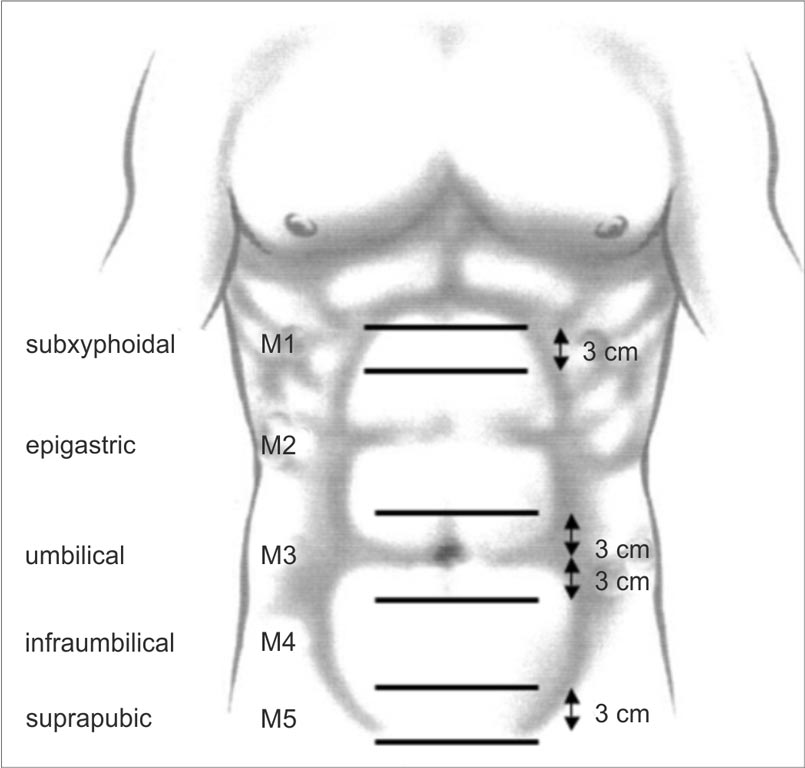
EHS recommends that the following parameters should be used for the classification of postoperative hernia: location of the defect, size (length and width) and whether it is a primary or reccurent hernia (fig. 1-4) (2).
EHS
Incisional Hernia Classification |
| Midline | subxiphoidal | M1 | |
| epigastric | M2 | |
| umbilical | M3 | |
| infraumbilical | M4 | |
| suprapubic | M5 | |
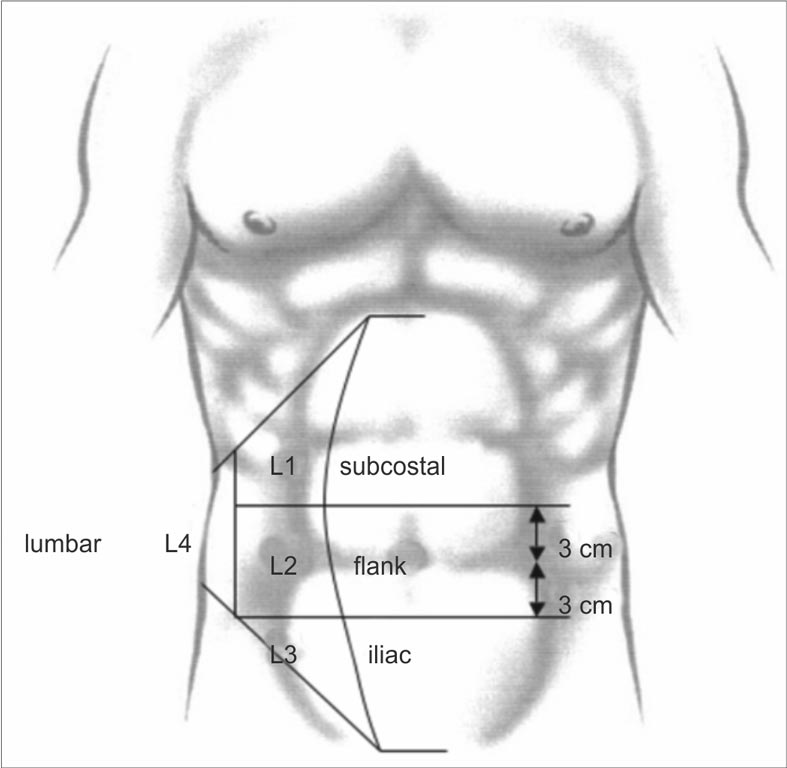
| Lateral | subcostal | L1 | |
| flank | L2 | |
| iliac | L3 | |
| lumbar | L4 | |
| Recurrent incisional hernia? | Yes O No O |
| length: cm | width: cm |
| Width cm | W1
< 4 cm
O | W2
> 4-10 cm
O | W3
> 10 cm
O |
Fig. 1. European Hernia Society classification for incisional abdominal wall hernias (2)
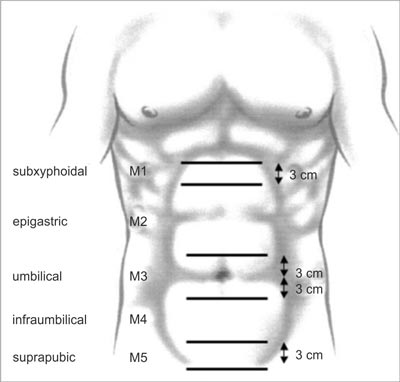
Fig. 2. To classify midline incisional hernias between the two lateral margins of the rectus muscle sheaths, five zones were defined (2)
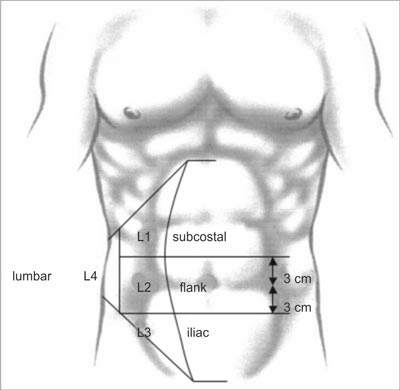
Fig. 3. To classify lateral incisional hernias, four zones lateral of the rectus muscle sheaths were defined (2)
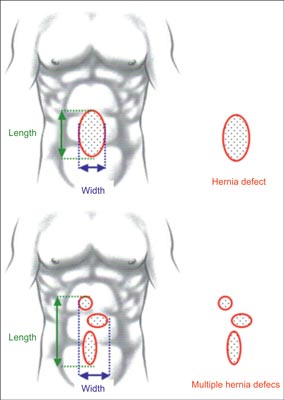
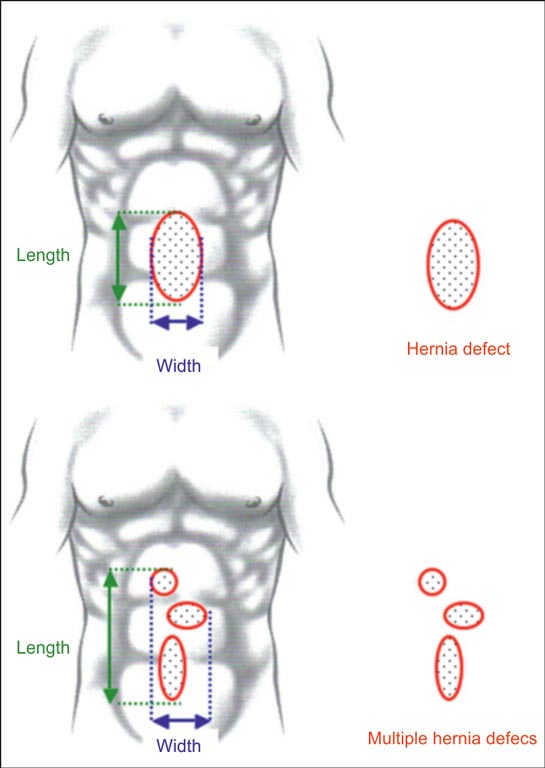
Fig. 4. Definition of the width and the length of incisional hernias for single hernia defects and multiple hernia defects (2)
In the literature, other classifications of postoperative hernia are available, including morphological classification of postoperative hernias (p / rxM ... S ... x ... RF ...):
• the character of hernia (p / rx) - primary / relapsing (x-number of relapses),
• location (M) - medial (m), perioceptal (u), suprapubic (sp), medial with narrow subcostal angle (m + sc), transcostal (sc), transverse (t), lumbar (l), medial (pm),
• size (S) [cm] - length x width,
• risk factors for relapse + for each factor (RF) - obesity (BMI > 25), male gender, nicotinism, operative wound contamination, age > 45 years, basic disease, 2 interventions within a month or > 2 within 1 year, complications during the postoperative period (7).
Clinical characteristics
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Poulose BK, Shelton J, Phillips S et al.: Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia 2012; 16: 179-183.
2. Muysoms FE, Miserez M, Berrevoet F et al.: Classification of primary and incisional abdominal wall hernias. Hernia 2009; 13(4): 407-414.
3. Korenkov M, Paul A, Sauerland S et al.: Classification and surgical treatment of incisional hernia. Results of an experts’ meeting. Langenbecks Arch Surg 2001; 386(1): 65-73.
4. Van’t Riet M, Steyerberg EW, Nellensteyn J et al.: Meta-analysis of techniques for closure of midline abdominal incisions. Br J Surg 2002; 89: 1350-1361.
5. Fortelny RH, Baumann P, Thasler WE et al.: Effect of suture technique on the occurrence of incisional hernia after elective midline abdominal wall closure: study protocol for a randomized controlled trial. Trials 2015; 16: 52.
6. Ah-kee EY, Kallachil T, O’Dwyer PJ: Patient awareness and symptoms from an incisional hernia. Int Surg 2014; 99(3): 241-246.
7. Dietz UA, Hamelmann W, Winkler MS et al.: An alternative classification of incisional hernias enlisting morphology, body type and risk factors in the assessment of prognosis and tailoring of surgical technique. J Plast Reconstr Aesthet Surg 2007; 60: 383-388.
8. Mitura K: Different approach to laparoscopic IPOM ventral hernia surgery – what has the last decade taught us? Pol Przegl Chir 2016; 88(1): 54-61.
9. Murphy KP, O’Connor OJ, Maher MM: Adult abdominal hernias. Am J Roentgenol 2014; 202(6): W506-W511.
10. Muysoms FE, Antoniou SA, Bury K et al.: European Hernia Society. European Hernia Society guidelines on the closure of abdominal wall incisions. Hernia 2015; 19(1): 1-24.
11. Murray BW, Cipher DJ, Pham T et al.: The impact of surgical site infection on the development of incisional hernia and small bowel obstruction in colorectal surgery. Am J Surg 2011; 202(5): 558-560.
12. Sørensen LT, Hemmingsen UB, Kirkeby LT et al.: Smoking Is a Risk Factor for Incisional Hernia. Arch Surg 2005; 140(2): 119-123.
13. Indrakusuma R, Jalalzadeh H, van der Meij JE et al.: Prophylactic Mesh Reinforcement versus Sutured Closure to Prevent Incisional Hernias after Open Abdominal Aortic Aneurysm Repair via Midline Laparotomy: A Systematic Review and Meta-Analysis. Eur J Vasc Endovasc Surg 2018; 56(1): 120-128.
14. Brosi P, Glauser PM, Speich B et al.: Prophylactic Intraperitoneal Onlay Mesh Reinforcement Reduces the Risk of Incisional Hernia, Two-Year Results of a Randomized Clinical Trial. World J Surg 2018; 42(6): 1687-1694.
15. Llaguna OH, Avgerinos DV, Nagda P et al.: Does Prophylactic Biologic Mesh Placement Protect Against the Development of Incisional Hernia in High-risk Patients? World J Surg 2011; 35: 1651-1655.
16. Verhelst J, Timmermans L, van de Velde M et al.: Watchful waiting in incisional hernia: is it safe? Surgery 2015; 157(2): 297-303.
17. Burger JWA, Luijendijk RW, Hop WCJ et al.: Long-term Follow-up of a Randomized Controlled Trial of Suture Versus Mesh Repair of Incisional Hernia. Ann Surg 2004; 240(4): 578-585.
18. Sugerman HJ, Kellum JM Jr, Reines HD et al.: Greater risk of incisional hernia with morbidly obese than steroid-dependent patients and low recurrence with prefascial polypropylene mesh. Am J Surg 1996; 171(1): 80-84.
19. Stetsko T, Bury K, Lubowiecka I et al: Safety and efficacy of a Ventralight ST echo ps implant for a laparoscopic ventral hernia repair – a prospective cohort study with a one-year follow-up. Pol Przegl Chir 2016; 88(1): 7-14.
20. Darehzereshki A, Goldfarb M, Zehetner J et al.: Biologic versus nonbiologic mesh in ventral hernia repair: a systematic review and meta-analysis. World J Surg 2014; 38(1): 40-50.
21. Rastegarpour A, Cheung M, Vardhan M et al.: Surgical mesh for ventral incisional hernia repairs: Understanding mesh design. Plast Surg (Oakv) 2016; 24(1): 41-50.
22. Bilsel Y, Abci I: The search for ideal hernia repair; mesh materials and types. Int J Surg 2012; 10(6): 317-321.
23. Bougard H, Coolen D, de Beer R et al.: HIG (SA) Guidelines for the management of ventral hernias. S Afr J Surg [Internet] 2016; 54(4): 1-32.
24. Timmermans L, de Goede B, van Dijk SM et al.: Meta-analysis of sublay versus onlay mesh repair in incisional hernia surgery. Am J Surg 2014; 207(6): 980-988.
25. Holihan JL, Nguyen DH, Nguyen MT et al.: Mesh location in open ventral hernia repair: a systematic review and network meta-analysis. World J Surg 2016; 40(1): 89-99.
26. Al Chalabi H, Larkin J, Mehigan B et al.: A systematic review of laparoscopic versus open abdominal incisional hernia repair, with meta-analysis of randomized controlled trials. Int J Surg 2015; 20: 65-74.
27. Froylich D, Segal M, Weinstein A et al.: Laparoscopic versus open ventral hernia repair in obese patients: a long-term follow-up. Surg Endosc 2016; 30(2): 670-675.
28. Eker HH, Hansson BME, Buunen M et al.: Laparoscopic vs Open Incisional Hernia Repair A Randomized Clinical Trial. JAMA Surg 2013; 148(3): 259-263.
29. Ratajczak A, Bobkiewicz A, Mitura K et al.: Posterior component separation – first report from Poland on new surgical technique used in major abdominal hernia treatment. Pol Przegl Chir 2016; 88(2): 118-123.
30. Rosen MJ, Jin J, McGee MF et al.: Laparoscopic component separation in the single-stage treatment of infected abdominal wall prosthetic removal. Hernia 2007; 11(5): 435-440.