Justyna Koszarska-Mirek, *Jakub Orleański
Abdominal desmoid-type fibromatosis – a case report and an overview of treatment options
Brzuszna postać fibromatozy – opis przypadku, przegląd metod terapeutycznych
Department of General Surgery with the Department of Oncological Surgery, The Independent Public Healthcare Facility in Świdnica
Head of Department: Adam Biernacki, PhD
Streszczenie
Fibromatoza (inaczej desmoid, guz desmoidalny, włókniakowatość) to nowotwór należący do grupy rozrostów tkanki włóknistej. Cechuje go brak możliwości dawania przerzutów odległych, lecz wykazuje miejscową złośliwość – agresywne naciekanie otaczających tkanek – i dużą skłonność do nawrotów po miejscowej resekcji.
Częstość występowania fibromatozy to 2-4 przypadki na milion osób w ciągu roku. Grupę desmoidów podzielono na formy: pozabrzuszną, brzuszną i wewnątrzbrzuszną. Najczęstsze postaci są sporadyczne, lecz obserwuje się współistnienie z zespołem rodzinnej polipowatości gruczolakowatej (FAP) tworzące zespół Gardnera. W terapii stosuje się: leczenie chirurgiczne, aktywną obserwację, hormonoterapię, niesteroidowe leki przeciwzapalne, chemioterapię, radioterapię.
Przedstawiony przypadek ma na celu zwrócenie uwagi na trudności w wyborze odpowiedniej terapii, ograniczenia leczenia chirurgicznego, aspekt psychologiczny schorzenia oraz konieczność aktywnego poszukiwania nowoczesnych rozwiązań diagnostyczno-leczniczych.
Autorzy prezentują przypadek 26-letniego pacjenta, u którego finalnie rozpoznano guz desmoidalny naciekający ściany oraz narządy wewnętrzne jamy brzusznej. Chory zgłosił się do szpitala powiatowego z podejrzeniem niedrożności przewodu pokarmowego. Z wywiadu uzyskano informację, iż wyczuł on u siebie guz powłok około 9 miesięcy przed przyjęciem.
Summary
Fibromatosis (desmoid, desmoid tumour) is a tumour belonging to the group of fibrous tissue proliferative diseases. Although the tumour cannot produce distant metastases, it shows local malignancy by invading adjacent tissues, as well as high recurrence rates after local resection.
The incidence of fibromatosis is 2-4 cases per 1 million inhabitants per year. Three types of fibromatosis have been distinguished: extra-abdominal, abdominal wall and intra-abdominal type. Although the most common types are sporadic, coexistence with familial adenomatous polyposis (FAP), known as the Gardner’s syndrome, is observed. Available therapeutic options include surgical treatment, watchful waiting, hormone therapy, non-steroid anti-inflammatory drugs, chemotherapy and radiation therapy.
This case report aims to draw attention to the difficulties in selecting an appropriate treatment option, limited surgical treatment, the psychological aspect of the disease, as well as the need to actively search for modern diagnostic and therapeutic solutions.
We present a case of a 26-year-old patient who was ultimately diagnosed with a desmoid tumour invading the abdominal wall and internal abdominal organs. The patient presented to a county hospital due to suspected gastrointestinal obstruction. It was found from medical history that the patient had palpated a tumour of the abdominal wall 9 months before admission.

Introduction
Fibromatosis (desmoid tumour) is an intermediate-grade tumour classified as a proliferative fibroblastic/myofibroblastic lesion (1), characterised by local malignancy in the form of aggressive invasion of adjacent tissues and frequent recurrence after surgical resection (2). These lesions do not produce distant metastases and do not form a pseudocapsule (2). Three types of fibromatosis have been distinguished: extra-abdominal (about 60%), abdominal wall (25%) and intra-abdominal (15%) type (2). Although suspicions can be raised based on imaging studies, histopathology is needed for the final diagnosis (1). The peak incidence of the disease is between 25 and 35 years of age, with an annual incidence of 2 to 4 new cases per million inhabitants; the disease is more common in women (3). Desmoid tumour should be differentiated with inflammatory myofibroblastoma, GIST, leiomyoma, leiomyosarcoma (LMS), low-grade fibromyxoid sarcoma (LGFMS), fibrosarcoma, a scar and a keloid (3). Fibromatosis may be also hereditary in about 10-25% of patients with familial adenomatous polyposis (FAP) (3). The coexistence of these two diseases is referred to as the Gardner’s syndrome, which is caused in most cases by a mutation in the APC tumor suppressor gene (3).
Case report
A 26-year-old male reported to a county hospital on the 11th March 2017 due to a 3-day abdominal pain and difficulty passing stool and gas. It was found from medical history that the patient had palpated a tumour in the abdominal cavity in the region of the left iliac fossa about 9 months before admission. Medical history of epilepsy and nicotine dependence. On admission, the patient was in good overall condition; physical examination revealed no abnormalities in the chest. The abdomen was soft, with no peritoneal symptoms. A large solid tumour about 12-14 cm in diameter was palpable in the left iliac fossa. Rectal examination revealed no abnormalities. Laboratory findings on admission revealed the following irregularities:
– Hgb 12.8 g/dL,
– neutrophil levels 80.5%,
– the presence of ketones in the urine,
– CRP 180.43 mg/L,
– sodium levels 133 mmol/L.
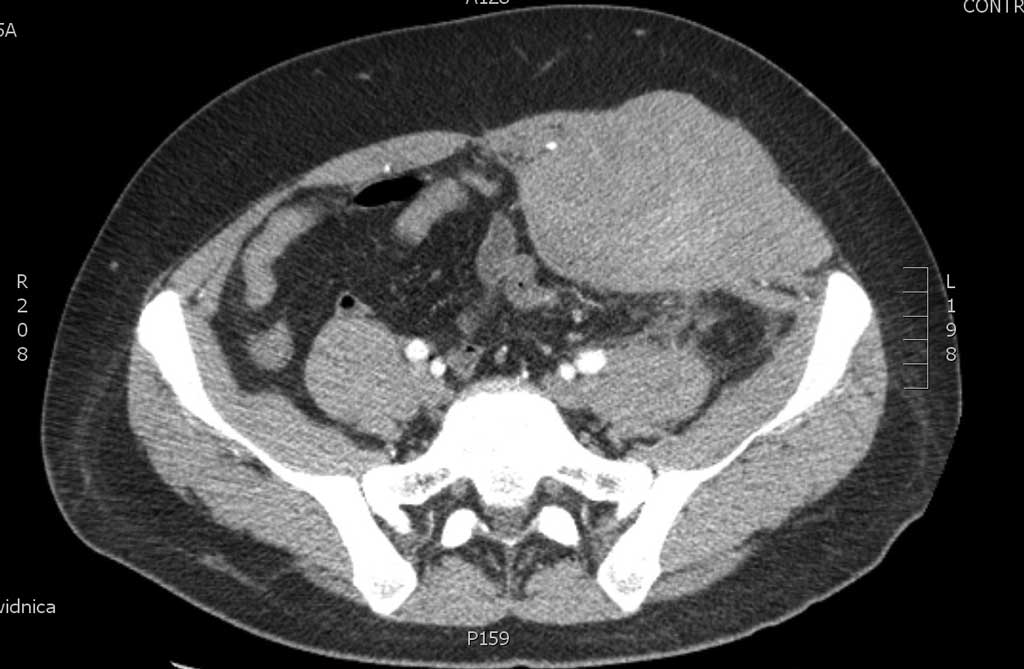
Abdominal CT excluded gastrointestinal obstruction, but showed infiltration of the distal descending colon and proximal sigmoid with thickened walls, bands of blurred adjacent adipose tissue, fluid and thickened peritoneal plaques. The infiltrative lesions reached the lateral abdominal wall at the level of lower abdomen with their blurring, followed by thickened oblique and rectus abdominis muscle on the left – to the maximum AP size of 88 mm – extending up to the level of the pubic symphysis. Inhomogeneous integumental areas – moderately hyperdense in an overview scan (fig. 1). Based on the correlation with the clinical picture, a tumour of the abdominal wall invading abdominal organs was diagnosed and the patient was referred to the Department of Soft Tissue Tumors for the biopsy of the infiltrative lesion of the abdominal wall.

Fig. 1. A CT image of the abdominal wall dated March 11, 2017
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Krzakowski M, Potemski P, Warzocha K, Wysocki P: Onkologia kliniczna. T. II. Via Medica, Gdańsk 2015.
2. Jeziorski A, Szawłowski A, Towpik E: Chirurgia onkologiczna. T. III. Wydawnictwo Lekarskie PZWL, Warszawa 2009.
3. Rutkowski P: Biblioteka chirurga onkologa. Mięsaki tkanek miękkich. Via Medica, Gdańsk 2015.
4. von Mehren M, Lor Randall R, Benjamin RS et al.: Soft tissue sarcoma. Version 1.2016. J Natl Compr Canc Netw 2016.
5. Kasper B: Systemic treatment approaches for sporadic desmoid-type fibromatosis: scarce evidence and recommendations. Oncol Res Treat 2015; 38(5): 244-248.
6. van Broekhoven DL, Deroose JP, Bonvalot S et al.: Isolated limb perfusion using tumour necrosis factor alpha and melphalan in patients with advanced aggressive fibromatosis. Br J Surg 2014; 101: 1674-1680.
7. Kujak JL, Liu PT, Johnson GB et al.: Early experience with percutaneous cryoablation of extra-abdominal desmoid tumors. Skeletal Radiol 2010; 39: 175-182.