© Borgis - Postępy Nauk Medycznych 4/2017, s. 201-205
*Ewa Kuklik, Michał Sojka, Łukasz Światłowski, Tomasz Roman, Anna Drelich-Zbroja, Małgorzata Szczerbo-Trojanowska
Bronchial artery embolization for the treatment of hemoptysis caused by Aspergillus fumigatus infection
Embolizacja tętnic oskrzelowych w leczeniu krwawień z dróg oddechowych spowodowanych infekcją Aspergillus fumigatus
Department of Interventional Radiology and Neuroradiology, Medical University in Lublin
Head of Department: Professor Małgorzata Szczerbo-Trojanowska, MD, PhD
Streszczenie
Wstęp. Aspergillus fumigatus jest jednym z najczęstszych patogenów będących przyczyną grzybiczej infekcji płucnej. Typowo występuje w postaci grzybniaka kropidlakowego płuc, będącego owalną masą złożoną ze splątanej grzybni kropidlaka. Często pierwszym i jedynym objawem choroby jest krwawienie z dróg oddechowych. Krwioplucie jest powikłaniem groźnym i bez leczenia szybko może doprowadzić do zgonu. Obecnie w leczeniu grzybniaków płuc możliwe jest zastosowanie nieinwazyjnych metod radiologii zabiegowej.
Cel pracy. Ocena skuteczności i bezpieczeństwa wewnątrznaczyniowej embolizacji tętnic oskrzelowych w leczeniu krwawień z dróg oddechowych będących powikłaniem inwazyjnej infekcji grzybiczej płuc.
Materiał i metody. Retrospektywnej analizie poddano badania 5 chorych leczonych z powodu grzybniaka płuc powikłanego krwawieniem z dróg oddechowych. W trzech przypadkach wykonano embolizację przy użyciu mikrosfer hydrożelowych, w dwóch przypadkach wykorzystano klej tkankowy.
Wyniki. Z powodu trudności technicznych u jednego chorego nie udało się zamknąć wszystkich naczyń. Pozostałe zostały prawidłowo zamknięte. Kontrolne badania angiograficzne u wszystkich chorych wykazały skuteczne zamknięcie embolizowanych naczyń i przetok. W ciągu sześciomiesięcznej obserwacji nie stwierdzono nawrotów krwawienia. Nie stwierdzono również żadnych powikłań związanych z zabiegiem embolizacji.
Wnioski. Embolizacja tętnic oskrzelowych jest bezpiecznym i skutecznym leczeniem krwawień z dróg oddechowych i zawsze powinna być rozważana jako leczenie w krwawieniach z grzybniaków płuc. Nie koliduje ona z leczeniem farmakologicznym i obie metody mogą być stosowane jednocześnie. W szczególnych przypadkach może być również zastosowana jako przygotowanie do zabiegu operacyjnego usunięcia płuc, zmniejszając znacznie ryzyko śmiertelności okołooperacyjnej.
Summary
Introduction. Aspergillus fumigatus is one of the most common fungal pathogens to cause lung infection. Typically, it presents in the form of aspergilloma, which is an oval mass consisted of matted mycelium. The first, and often the only symptom is bleeding from the respiratory tract. Hemoptysis is a dangerous complication, without treatment can quickly lead to death. Currently, interventional radiology gives a possibility of non-invasive treatment in hemoptysis caused by aspergilloma infection.
Aim. Evaluation the efficacy and safety of endovascular embolization of the bronchial arteries for the treatment of haemoptysis, which is a complication of invasive fungal infection of the lungs.
Material and methods. The study was a retrospective analysis of 5 patients treated due to hemoptysis as a complication of pulmonary aspergilloma. In three cases, embolization was performed using hydrogel microspheres, in two cases a tissue glue was used.
Results. In one case, due to technical difficulties, complete embolization wasn’t possible. Others have been properly closed. Control angiographic examinations showed effective closure of embolized arteries. In the six-month follow-up there was no recurrence of bleeding, there were also no complications related to the embolization procedure.
Conclusions. Bronchial artery embolization is a safe and effective treatment of bleeding from the respiratory tract and should always be considered as a treatment option for haemoptysis caused by aspergilloma. The procedure does not interfere with pharmacological therapy, and both methods can be used simultaneously. In special cases, it can also be used as preparation for surgery, significantly reducing the risk of perioperative mortality.

INTRODUCTION
Aspergillus fumigatus is one of the most common fungal pathogens to cause pulmonary infection. The fungal spores can be inhaled to the lungs or moved to the bloodstream with surgical tools and lead to generalized infection of the body (1).
Aspergillus fumigatus infection may have different forms, from allergic to invasive pulmonary aspergillosis (2). The most common form of A. fumigatus infection is aspergilloma which is an oval mass consisting of tangled mycelium. Mycetoma usually develops in patients with no immune deficiencies. The sole condition of aspergilloma growth is the presence of pulmonary cavities, predominantly postinflammatory, sarcoidosic or bronchiectatic cavitary lesions (3).
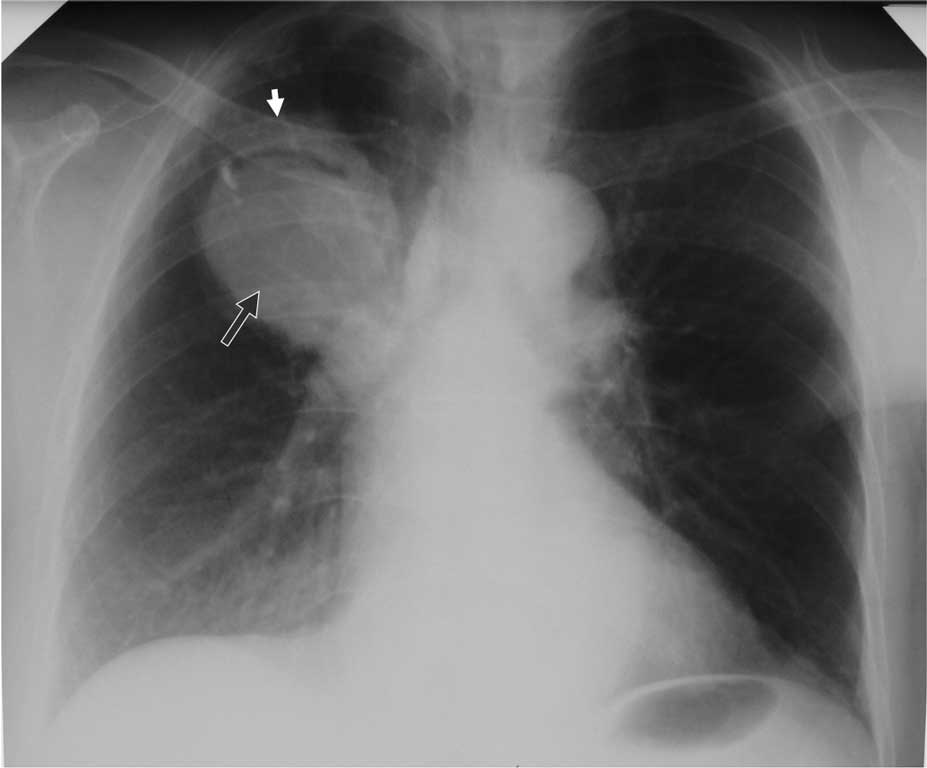
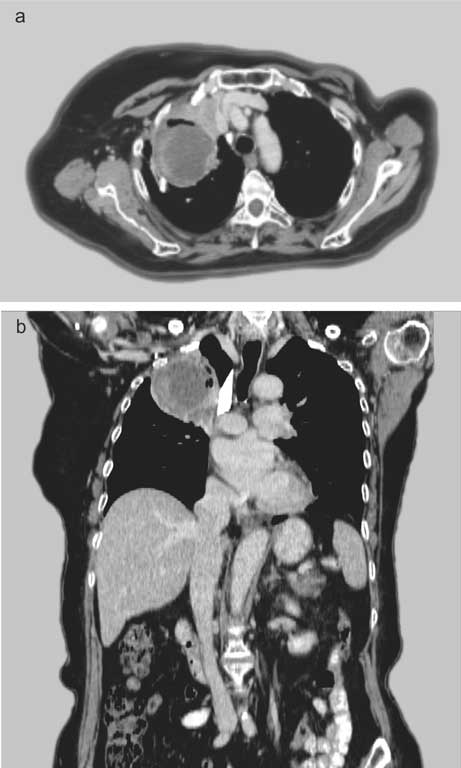
The major radiographic finding in aspergilloma is a characteristic oval shadow in the lung cavity surrounded by air and the cavity wall (fig. 1, 2a, b). To confirm the diagnosis, tests for A. fumigatus antibodies can be performed (4, 5).

Fig. 1. Oval mass (black arrow) with characteristic ring (white arrow) in the upper lobe of the right lung
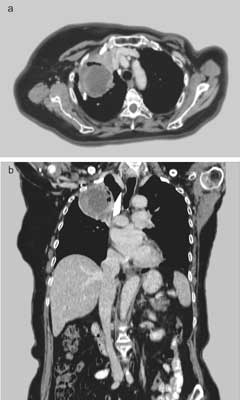
Fig. 2a, b. Aspergilloma in CT
The most dangerous and often the only symptom of aspergilloma is bleeding from the respiratory tract. Haemoptysis occurs due to congestion and increased pressure in the inflamed vessels, ultimately resulting in rupture of the vessel wall and extravasation. The other damaging factors are proteolytic enzymes produced by the scraps of a growing mycelium. The main cause of death in patients with haemoptysis is asphyxia. Direct consequences in the form of massive haemorrhage are extremely rare (6, 7).
Nowadays, thanks to advances in interventional radiology, dangerous bleedings from the bronchial tree can be treated with percutaneous, minimally invasive bronchial artery embolization (BAE).
AIM
The aim of this study was to evaluate the efficacy and safety of endovascular embolization of the bronchial arteries for the treatment of haemoptysis, which is a complication of invasive fungal infection of the lungs.
MATERIAL AND METHODS
In the retrospective study, 5 cases of patients with aspergilloma complicated by bleeding from the airway treated in the Department of Radiology and Neuroradiology from September 2011 to September 2016, were analysed. The study group consisted of 20% of women and 80% of men, aged 50-80 years. Four patients were treated previously for tuberculosis, one patient was diagnosed with throat cancer. The diagnosis was based on chest X-ray and computed tomography (CT) scans. Aspergillomas were detected in the form of a tumour growing in the lung cavity, whose boundaries were visible through the gas limbus separating the tumour mass from the lung cavity, called the Monad’s sign.
Embolization procedures were performed at the Department of Radiology and Neuroradiology MU in Lublin, using a Siemens Multi Star system. The procedures were performed under local anaesthesia. The Seldinger method was applied to puncture the femoral artery. The vascular 5 French sheath was inserted. Aortography was performed using a Pigtail catheter and a contrast agent Visipaque 320 administered in a volume of 25 ml with the flow rate of 12 ml/sec. Once the presence of pathological vessels was confirmed, embolisation was performed.
RESULTS
Vessels supplying the mycetomas were intercostal and bronchial arteries as well as branches of the internal mammary artery. Arteries were selectively cannulated. Depending on the anatomical conditions, different catheters were used, most commonly Pigtail, Cobra, Simmonds1, Simmonds2 and Progreat microcatheters (Terumo).
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Ebby O: Community-Acquaired Pneumonia: From Common Pathogens To Emerging Resistance. Emerg Med Pract 2005; 7(12): 1-24.
2. Maskell N, Millar A (eds.): Oxford desk reference. Respiratory Medicine. University Press, Oxford 2009: 196.
3. Herbrecht R, Denning D, Patterson T: Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillus Study Group. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med 2002; 347(6): 408-415.
4. Patterson K: Diagnosis and Treatment of Pulmonary Aspergillosis Syndromes. Chest 2014; 146(5): 1358-1368.
5. Shifren A (ed.): The Washington Manual Pulmonary Medicine Subspecialty Consult. Lippincott Williams & Wilkins 2006: 96-106.
6. Reichenberger F, Habicht JM, Gratwohl A, Tamm M: Diagnosis and treatment of invasive pulmonary aspergillosis in neutropenic patients. Eur Respir J 2002; 19: 743-755.
7. Srivastava D, Manisha J, Bhalla A et al.: Bronchial Artery Embolization in Pulmonary Diseases: Current Scenario. JIMSA 2013; 26(1): 69-71.
8. Rashad A, Amin M, El-Azim A: Percutaneous transcatheter vascular embolization for life threatening hemoptysis. Egypt J Chest Dis Tuberc 2013; 62: 755-759.
9. Remy J, Voisin C, Ribet M: Treatment by embolization of severe or repeated hemoptysis associated with systemic hypervascularization. Nouv Presse Med 1973; 2: 2060-2068.
10. Serasli E, Kalpakidis V, Iatrou K et al.: Percutaneous bronchial artery embolization in the management of massive hemoptysis in chronic lung diseases. Immediate and long-term outcomes. Interv Oncol 2008 Aug; 27(4): 319-328.
11. Ding WY, Chan T, Yadavilli RK, McWilliams R: Aspergilloma and massive haemoptysis. BMJ Case Report 2014 Apr 16; 2014. pii: bcr2013200019.
12. Corr P: Management of severe hemoptysis from pulmonary aspergilloma using endovascular embolization. Cardiovasc Intervent Radiology 2006 Sep-Oct; 29(5): 807-810.